ICD-10 code C18. 7 for Malignant neoplasm of sigmoid colon is a medical classification as listed by WHO under the range - Malignant neoplasms .
Full
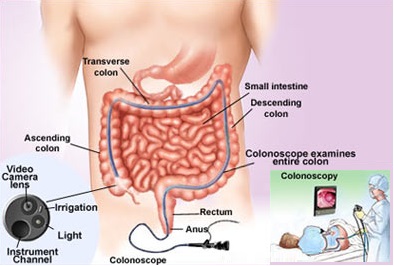
AnswerCan colon cancer be detected by sigmoidoscopy?
The test can also look for evidence of inflammation or cancer of the rectum and lower colon. Sigmoidoscopy can also be used to remove small fleshy lumps (polyps) that can be found in the colon and take samples of tissue (biopsy) for analysis. This is done by passing a thin 'grabbing' instrument down a side channel of the sigmoidoscope.
What are some symptoms of colon and rectal cancer?
- A change in bowel habits, such as diarrhea, constipation, or narrowing of the stool, that lasts for more than a few days
- A feeling that you need to have a bowel movement that's not relieved by having one
- Rectal bleeding with bright red blood
- Blood in the stool, which might make the stool look dark brown or black
- Cramping or abdominal (belly) pain
What is the diagnosis code for cancer?
carcinoma in (M8220/3) 153.9. 153.8. ICD9Data.com. 154. ICD-9-CM codes are used in medical billing and coding to describe diseases, injuries, symptoms and conditions. ICD-9-CM 153.9 is one of thousands of ICD-9-CM codes used in healthcare.
Is adenocarcinoma of the colon curable?
While metastatic adenocarcinoma may not be curable, it is treatable, and treatments can often both extend a patient's life expectancy and reduce the symptoms of cancer. With treatments improving rapidly, it's hard for anyone to stay on top of all of the research.
What is the ICD-10 code for sigmoid colon cancer?
ICD-10 code: C18. 7 Malignant neoplasm: Sigmoid colon.
What is the ICD-10-CM code for colon cancer?
C18. 9 - Malignant neoplasm of colon, unspecified. ICD-10-CM.
What is the ICD-10 code for sigmoid mass?
7: Malignant neoplasm of sigmoid colon.
What is diagnosis code C18 9?
ICD-10 code: C18. 9 Malignant neoplasm: Colon, unspecified.
Is Z12 11 a primary diagnosis code?
If the patient presents for a screening colonoscopy and a polyp or any other lesion/diagnosis is found, the primary diagnosis is still going to be Z12. 11, Encounter for screening for malignant neoplasm of colon. The coder should also report the polyp or findings as additional diagnosis codes.
What does Z12 31 mean?
For example, Z12. 31 (Encounter for screening mammogram for malignant neoplasm of breast) is the correct code to use when you are ordering a routine mammogram for a patient. However, coders are coming across many routine mammogram orders that use Z12. 39 (Encounter for other screening for malignant neoplasm of breast).
Where is the sigmoid colon located in the abdominal cavity?
The sigmoid colon is an “S” shaped portion of the large intestine that begins in front of the pelvic brim as a continuation of the descending colon and becomes the rectum at the level of the third sacral vertebrae.
What is the ICD 10 code for thickening of the sigmoid colon?
89.
What is the ICD 10 code for colon mass?
2022 ICD-10-CM Diagnosis Code C18. 9: Malignant neoplasm of colon, unspecified.
What is malignant neoplasm of colon?
The term "malignant neoplasm" means that a tumor is cancerous. A doctor may suspect this diagnosis based on observation — such as during a colonoscopy — but usually a biopsy of the lesion or mass is needed to tell for sure whether it is malignant or benign (not cancerous).
What is colorectal code?
Metastasis to the colon or rectum is classified to code 197.5. Carcinoma of the colon is assigned to code 230.3 while carcinoma of the rectum goes to 230.4.
What is metastatic colorectal adenocarcinoma?
Summary. Metastatic colorectal cancer is advanced cancer that has spread to other areas outside the colon and rectum. Commonly, this type of cancer spreads to the lymph nodes and liver, but it may spread to other parts of the body, such as the brain.
What are adenocarcinoma cells?
Adenocarcinoma develops in cells located in the glands that line your organs (glandular epithelial cells). These cells secrete mucous, digestive juices or other liquids. If your glandular cells begin to change or grow out of control, tumors can form. Some tumors found in glandular cells are not cancerous.
What is colonic new growth?
Colonic polyps, also known as colorectal polyps, are growths that appear on the surface of the colon. The colon, or large intestine, is a long hollow tube at the bottom of the digestive tract. It's where the body makes and stores stool.
How long is Hemicolectomy surgery?
A hemicolectomy usually takes about two hours, but it may take longer depending on any complications during the procedure.
What is the ICD-10 code for liver metastasis?
ICD-10 code: C78. 7 Secondary malignant neoplasm of liver and intrahepatic bile ducts.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
When will the ICD-10 C18.7 be released?
The 2022 edition of ICD-10-CM C18.7 became effective on October 1, 2021.
What is a type 1 exclude note?
A type 1 excludes note is a pure excludes. It means "not coded here". A type 1 excludes note indicates that the code excluded should never be used at the same time as C18.7. A type 1 excludes note is for used for when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
What is the convention of ICd 10?
The conventions for the ICD-10-CM are the general rules for use of the classification independent of the guidelines. These conventions are incorporated within the Alphabetic Index and Tabular List of the ICD-10-CM as instructional notes.
When to assign Y to ICD-10?
two separate conditions classified to the same ICD-10-CM diagnosis code): Assign “Y” if all conditions represented by the single ICD-10-CM code were present on admission (e.g. bilateral unspecified age-related cataracts).
What is code assignment?
Code assignment is based on the provider’s documentation of the relationship between the condition and the care or procedure, unless otherwise instructed by the classification. The guideline extends to any complications of care, regardless of the chapter the code is located in. It is important to note that not all conditions that occur during or following medical care or surgery are classified as complications. There must be a cause-and-effect relationship between the care provided and the condition, and an indication in the documentation that it is a complication. Query the provider for clarification, if the complication is not clearly documented.
When to use counseling Z code?
Counseling Z codes are used when a patient or family member receives assistance in the aftermath of an illness or injury , or when support is required in coping with family or social problems. They are not used in conjunction with a diagnosis code when the counseling component of care is considered integral to standard treatment.
When assigning a chapter 15 code for sepsis complicating abortion, pregnancy, childbirth, and the?
When assigning a chapter 15 code for sepsis complicating abortion, pregnancy, childbirth, and the puerperium, a code for the specific type of infection should be assigned as an additional diagnosis. If severe sepsis is present, a code from subcategory R65.2, Severe sepsis, and code(s) for associated organ dysfunction(s) should also be assigned as additional diagnoses.
Which code should be sequenced first?
code from subcategory O9A.2, Injury, poisoning and certain other consequences of external causes complicating pregnancy, childbirth, and the puerperium, should be sequenced first, followed by the appropriate injury, poisoning, toxic effect, adverse effect or underdosing code, and then the additional code(s) that specifies the condition caused by the poisoning, toxic effect, adverse effect or underdosing.
Do not code diagnoses documented as “probable”, “suspected,” “questionable,” “?
Do not code diagnoses documented as “probable”, “suspected,” “questionable,” “rule out ,” or “working diagnosis” or other similar terms indicating uncertainty. Rather, code the condition(s) to the highest degree of certainty for that encounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit.
What is the synonym for cancer of the colon?
Malignant neoplasm of colon. Approximate Synonyms. Cancer of the colon. Cancer of the colon, adenocarcinoma. Cancer of the colon, hereditary nonpolyposis. Cancer of the colon, stage 1. Cancer of the colon, stage 2. Cancer of the colon, stage 3. Cancer of the colon, stage 4.
What is a primary or metastatic malignant neoplasm that affects the colon?
A primary or metastatic malignant neoplasm that affects the colon. Representative examples include carcinoma, lymphoma, and sarcoma.
What is malignant tumor?
Malignant tumor of colon. Metastasis from malignant tumor of colon. Primary adenocarcinoma of colon. Clinical Information. A primary or metastatic malignant neoplasm involving the colon. A primary or metastatic malignant neoplasm that affects the colon or rectum.
When will the ICD-10 C18.9 be released?
The 2022 edition of ICD-10-CM C18.9 became effective on October 1, 2021.
Can multiple neoplasms be coded?
For multiple neoplasms of the same site that are not contiguous, such as tumors in different quadrants of the same breast, codes for each site should be assigned. Malignant neoplasm of ectopic tissue. Malignant neoplasms of ectopic tissue are to be coded to the site mentioned, e.g., ectopic pancreatic malignant neoplasms are coded to pancreas, ...
What is the code for colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code Z12.11 ( encounter for screening for malignant neoplasm of the colon ).
What is G0121 in medical terms?
G0121 ( colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk.
What is the Difference between a Screening Test and a Diagnostic Colonoscopy?
A screening test is a test provided to a patient in the absence of signs or symptoms based on the patient’s age, gender, medical history and family history according to medical guidelines. It is defined by the population on which the test is performed, not the results or findings of the test.
How often can you get a colonoscopy with Medicare?
Medicare beneficiaries without high risk factors are eligible for screening colonoscopy every ten years. Beneficiaries at high risk for developing colorectal cancer are eligible once every 24 months. Medicare considers an individual at high risk for developing colorectal cancer as one who has one or more of the following:
What is a colonoscopy screening?
As such, “screening” describes a colonoscopy that is routinely performed on an asymptomatic person for the purpose of testing for the presence of colorectal cancer or colorectal polyps. Whether a polyp or cancer is ultimately found does not ...
What is a G0121?
Colonoscopy, flexible, proximal to splenic flexure; diagnostic, with or without collection of specimen (s) by brushing or washing, with or without colon decompression (separate procedure) G0121 ( colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk.
What are the global periods for colonoscopy?
Typically, procedure codes with 0, 10 or 90-day global periods include pre-work, intraoperative work, and post-operative work in the Relative Value Units (RVUs) assigned . As a result, CMS’ policy does not allow for payment of an Evaluation and Management (E/M) service prior to a screening colonoscopy. In 2005, the Medicare carrier in Rhode Island explained the policy this way:

Popular Posts:
- 1. icd 10 code for acute tabular necrosis
- 2. icd 10 code for aftercare craniotomy
- 3. icd 10 code for pediatric physical with no abnormal finding
- 4. icd 10 code for peg tube dependence
- 5. icd-10 code for history of benign neoplasm
- 6. icd 10 code for abnormal cat scan of abdomen
- 7. icd 10 code for poor compliance
- 8. icd 10 code for ganlion cyst wrist
- 9. what is the icd 10 code for spinal fusion
- 10. injected with dye for an intravenous pyelogram icd 10 cm code