Full Answer
How do you code recurrent UTI?
- Date of Admission
- Date (s) of indwelling urinary catheter insertion/removal if applicable
- Is patient >65 years of age?
- Collection date (s) and results of urine cultures including colony count
- Date (s) and types of UTI sign/symptoms
- Collection date (s) and results of any positive blood cultures
What is the ICD 10 code for UTI?
ICD-10-CM Code N39.0
- MS-DRG - Medicare Severity-Diagnosis Related Group
- Clinical Concepts. The code N39.0 can also be found in the following clinical concepts.
- Coding structure: Should you use N39.0 or N390 ( with or without decimal point )? DO NOT include the decimal point when electronically filing claims as it may be rejected.
What is the CPT code for UTI?
N39.0 - Urinary tract infection, site not specified N39.3 - Stress incontinence (female) (male) N39.4 - Other specified urinary incontinence N39.41 - Urge incontinence N39.42 - Incontinence without sensory awareness N39.43 - Post-void dribbling N39.44 - Nocturnal enuresis N39.45 - Continuous leakage
How is urinary tract infection (UTI) diagnosed?
- Infections of the urinary tract are one of the most frequent reasons for treatment in primary medical care.
- Diagnosis solely based on clinical symptoms is often wrong.
- Asymptomatic bacteriuria only requires treatment in exceptional cases.
- Diagnostic precision can be increased by using dip sticks and clinical algorithms.
What is the ICD-10 diagnosis code for sepsis due to UTI?
The ED coder would assign the following ICD-10 diagnosis codes:R65.21Severe sepsis with shockN39.0UTI, site not specifiedR30.0DysuriaR50.81Fever presenting with conditions classified elsewhereN17.9Acute kidney failure, unspecified2 more rows
How do you code sepsis for UTI?
A41. 51 (Sepsis due to Escherichia coli), and N39. 0 (Urinary tract infection, site not specified) would be reported as additional diagnoses.
What is the ICD-10 code for sepsis due to E coli?
ICD-10 code A41. 51 for Sepsis due to Escherichia coli [E. coli] is a medical classification as listed by WHO under the range - Certain infectious and parasitic diseases .
What is the ICD-10 code for bacterial sepsis?
ICD-10-CM Code for Sepsis, unspecified organism A41. 9.
Do you code sepsis first or UTI?
0-, Infection following immunization, should be coded first, followed by the code for the specific infection. If the patient has severe sepsis, the appropriate code from subcategory R65. 2 should also be assigned, with the additional codes(s) for any acute organ dysfunction.
What is the difference between urosepsis and sepsis?
Sepsis is a systemic inflammatory response to infection that can lead to multi-organ dysfunction, failure, and even death. Urosepsis is sepsis caused by infections of the urinary tract, including cystitis, or lower urinary tract and bladder infections, and pyelonephritis, or upper urinary tract and kidney infections.
When do you code sepsis?
Severe sepsis requires at least 2 ICD-10-CM codes; a code for the underlying systemic infection and a code from category R65. 2 Severe Sepsis; you should also assign a code(s) for the acute organ dysfunction if documented; Codes R65. 20 and R65.
What is the ICD-10 code for severe sepsis with septic shock?
ICD-10 Code for Severe sepsis with septic shock- R65. 21- Codify by AAPC.
Can sepsis be coded as primary diagnosis?
According to the guidelines above, sepsis would be the appropriate principal diagnosis if it is the reason the patient is admitted, and meets the definition of principal diagnosis.
Do you code questionable sepsis?
1. d.a states that R65. 2- can be coded when severe sepsis or an associated organ dysfunction is documented. If “severe sepsis” is documented without mention of organ dysfunction, R65.
When coding sepsis and severe sepsis which code should be sequenced first?
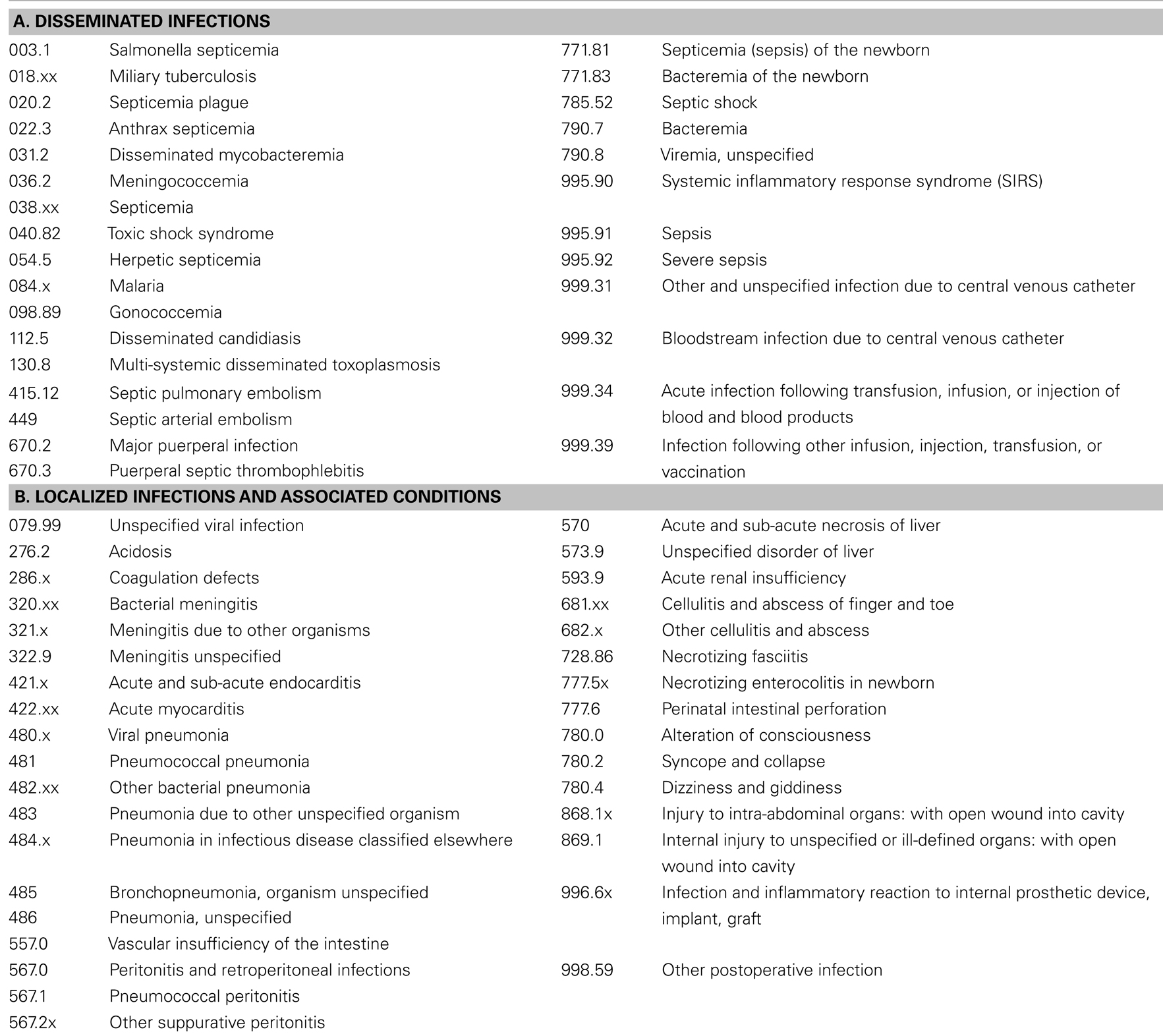
If the patient's reason for admission is sepsis or severe sepsis or SIRS and a localized infection such as cellulitis, the code for the systemic infection is sequenced first, followed by code 995.91 or 995.92, then the code for the localized infection.
What is sepsis unspecified?
Overview. Sepsis is a potentially life-threatening condition that occurs when the body's response to an infection damages its own tissues. When the infection-fighting processes turn on the body, they cause organs to function poorly and abnormally. Sepsis may progress to septic shock.
What is systemic disease?
Systemic disease associated with the presence of pathogenic microorganisms or their toxins in the blood. The presence of pathogenic microorganisms in the blood stream causing a rapidly progressing systemic reaction that may lead to shock. Symptoms include fever, chills, tachycardia, and increased respiratory rate.
What is the term for the presence of bacteria or their toxins in the blood or tissues?
Urosepsis . Clinical Information. (sep-sis) the presence of bacteria or their toxins in the blood or tissues. A disorder characterized by the presence of pathogenic microorganisms in the blood stream that cause a rapidly progressing systemic reaction that may lead to shock.
Why is severe sepsis not assigned?
For instance, if sepsis, pneumonia, and acute renal failure due to dehydration are documented, the code for severe sepsis may not be assigned because the acute renal failure is not stated as due to or associated with sepsis. If the documentation is unclear, query the physician.
What is the most common type of infection that leads to sepsis?
Localized Infection. Almost any type of infection can lead to sepsis. Infections that lead to sepsis most often start in the lung, urinary tract, skin, or gastrointestinal tract. When localized infections are contained, they tend to be self-limiting and resolve with antibiotics.
How does sepsis affect the body?
Sepsis is an extreme response to infection that develops when the chemicals the immune system releases into the bloodstream to fight infection cause widespread inflammation. This inflammation can lead to blood clots and leaky blood vessels, and without timely treatment, may result in organ dysfunction and then death. Severe cases of sepsis often result from a body-wide infection that spreads through the bloodstream, but sepsis can also be triggered by an infection in the lungs, stomach, kidneys, or bladder. Thus, it is not necessary for blood cultures to be positive to code sepsis (guideline I.C.1.d.1.a.i).
How to improve sepsis documentation?
To improve sepsis documentation, coding staff needs to work closely with clinical documentation improvement specialists (CDIs), and everyone must be clear on what documentation is needed to correctly code sepsis. A physician champion can be helpful to establish guidelines for the physicians and standard terminology to use when documenting sepsis. A coding tip sheet that includes various scenarios is a helpful tool for the coding department to standardize definitions and the interpretation of the coding guidelines. A regular audit of sepsis DRGs or sepsis as a secondary code can help to identify documentation issues and coders who need more education. Sepsis is never going to be easy to code, but with continuous education and teamwork across departments, the sepsis beast can be conquered.
What is septic shock?
Septic shock refers to circulatory failure associated with severe sepsis. It is a life-threatening condition that happens when the exaggerated response to infection leads to dangerously low blood pressure (hypotension). Septic shock is a form of organ failure.
When is a localized infection coded?
If the patient is admitted with a localized infection and the patient does not develop sepsis or severe sepsis until after the admission, the localized infection is coded first, followed by the appropriate codes for sepsis or severe sepsis, if applicable .
What are the symptoms of a localized infection?
Documentation issues: A patient with a localized infection usually presents with tachycardia, leukocytosis, tachypnea, and/or fever. These are typical symptoms of any infection. It is up to the clinical judgment of the physician to decide whether the patient has sepsis.

Popular Posts:
- 1. icd 10 code for hemophylia
- 2. icd 10 code for emphysema and copd
- 3. icd 10 cm code for h. zoster
- 4. icd 10 cm code for cellulitis of abdominal wall
- 5. icd 10 dx code for dehydration
- 6. in icd 10, for physical therapy following a fracture, what is the encounter code
- 7. icd 10 code for renal colic right side
- 8. icd 10 code for left occipital fracture
- 9. icd 10 code for diverticular abcess
- 10. icd 10 pcs code for external chest compressions for 20 minutes unsuccessful