Malignant neoplasm of unspecified kidney, except renal pelvis. C64.9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2019 edition of ICD-10-CM C64.9 became effective on October 1, 2018.
Malignant neoplasm of unspecified kidney, except renal pelvis . C64. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
Full
Answerrenal pelvis
The renal pelvis or pelvis of the kidney is the funnel-like dilated part of the ureter in the kidney. In humans, the renal pelvis is the point where the two or three major calyces join.
https://en.wikipedia.org › wiki › Renal_pelvis
What is the survival rate for renal cancer?
This number compares people with the same stage of kidney cancer to people without cancer 5 years after diagnosis. The 5-year survival rate for all types of kidney cancer combined is 75%. That means you’re 75% as likely to live at least 5 years as people who don’t have cancer.
What are the types of kidney cancer?
What Is Kidney Cancer?
- The kidneys. The kidneys are a pair of bean-shaped organs, each about the size of a fist. ...
- Types of kidney cancer. Renal cell carcinoma (RCC), also known as renal cell cancer or renal cell adenocarcinoma, is the most common type of kidney cancer.
- Benign (non-cancerous) kidney tumors. Some kidney tumors are benign (non-cancer). ...
What is the ICD 10 for end stage renal disease?
End stage renal disease N18. 6 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2020 edition of ICD-10-CM N18.
What is the treatment for renal cancer?
Treatment for renal cancer Surgery Surgery to remove part or all of the kidney is often used to treat renal cell cancer. The following types of surgery may be used: • Partial nephrectomy: A surgical procedure to remove the cancer within the kidney and some of the tissue around it. A partial nephrectomy may be done
What is the ICD-10 code for kidney cancer?
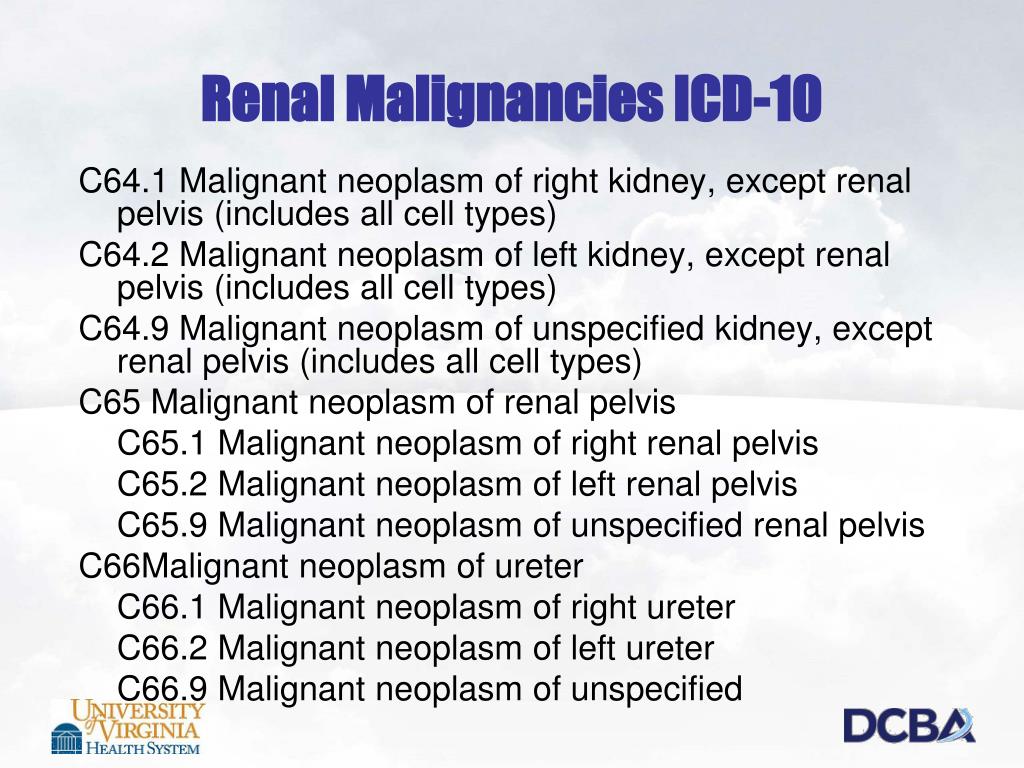
Kidney Cancer – Renal Cell Carcinoma (ICD-10: C64)
What is the ICD-10 code for right kidney cancer?
ICD-10 Code for Malignant neoplasm of right kidney, except renal pelvis- C64. 1- Codify by AAPC.
How do you code renal cell carcinoma?
Renal cell carcinoma (8312) is a group term for glandular (adeno) carcinomas of the kidney.
What is the ICD-10 code for personal history of renal cancer?
Z85. 528 - Personal history of other malignant neoplasm of kidney | ICD-10-CM.
What are the ICD-10 codes for cancer?
International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version for 2010C00-C97 Malignant neoplasms. ... D00-D09 In situ neoplasms.D10-D36 Benign neoplasms.D37-D48 Neoplasms of uncertain or unknown behaviour.
What is malignant neoplasm of kidney?
Renal cell cancer (also called kidney cancer or renal cell adenocarcinoma) is a disease in which malignant (cancer) cells are found in the lining of tubules (very small tubes) in the kidney. There are 2 kidneys, one on each side of the backbone, above the waist. Tiny tubules in the kidneys filter and clean the blood.
What is the ICD 9 code for renal cell carcinoma?
ICD-9 Code 189.0 -Malignant neoplasm of kidney except pelvis- Codify by AAPC.
Is renal cell carcinoma a solid tumor?
Solid tumors of the kidney are rare - approximately three-fourths of these tumors are cancerous with the potential to spread. The most common types of kidney cancer include: Renal cell carcinoma (adenocarcinoma) Wilm's tumor (nephroblastoma)
What is metastatic renal cell carcinoma?
Metastatic renal cell carcinoma is cancer in your kidneys that has spread to other parts of your body. It's also called stage IV renal cell cancer. Cancer is harder to treat after it spreads, but it's not impossible.
What is the ICD-10 code for History of nephrectomy?
5: Acquired absence of kidney.
What is the ICD-10 code for metastatic renal cell carcinoma?
Secondary malignant neoplasm of unspecified kidney and renal pelvis. C79. 00 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C79.
Where does renal cell carcinoma originate from?
Renal cell carcinoma (RCC) is a kidney cancer that originates in the lining of the proximal convoluted tubule, a part of the very small tubes in the kidney that transport primary urine. RCC is the most common type of kidney cancer in adults, responsible for approximately 90–95% of cases.
Is renal cell carcinoma an adenocarcinoma?
Renal cell carcinoma (RCC), also known as renal cell cancer or renal cell adenocarcinoma, is the most common type of kidney cancer. About 9 out of 10 kidney cancers are renal cell carcinomas.
What is stage 4 renal cell carcinoma?
Stage 4 is the most advanced form of the disease. Stage 4 means that the cancer has spread to the adrenal gland or has spread to distant lymph nodes or other organs. Because the adrenal gland is attached to the kidney, the cancer often spreads there first.
What is the ICD 10 code for metastatic renal cell carcinoma?
Secondary malignant neoplasm of unspecified kidney and renal pelvis. C79. 00 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C79.
What causes renal cell carcinoma?
Causes. The exact cause of renal cell carcinoma is not known. However, a history of smoking does increase the risk for developing this disease. Patients with von Hippel-Lindau disease, horseshoe kidneys, adult polycystic kidney disease and kidney failure are also more prone to develop renal cell carcinoma.
What is the ICd 10-CM tabular list?
The ICD-10-CM Tabular List contains categories, subcategories and codes. Characters for categories, subcategories and codes may be either a letter or a number. All categories are 3 characters. A three-character category that has no further subdivision is equivalent to a code. Subcategories are either 4 or 5 characters. Codes may be 3, 4, 5, 6 or 7 characters. That is, each level of subdivision after a category is a subcategory. The final level of subdivision is
What is the convention of ICd 10?
The conventions for the ICD-10-CM are the general rules for use of the classification independent of the guidelines. These conventions are incorporated within the Alphabetic Index and Tabular List of the ICD-10-CM as instructional notes.
What does NEC mean in coding?
NEC “Not elsewhere classifiable” This abbreviation in the Alphabetic Index represents “other specified.”When a specific code is not available for a condition, the Alphabetic Index directs the coder to the “other specified” code in the Tabular List.
How to select a code in the classification that corresponds to a diagnosis or reason for visit documented in a?
To select a code in the classification that corresponds to a diagnosis or reason for visit documented in a medical record, first locate the term in the Alphabetic Index, and then verify the code in the Tabular List. Read and be guided by instructional notations that appear in both the Alphabetic Index and the Tabular List.
When to assign Y to ICD-10?
two separate conditions classified to the same ICD-10-CM diagnosis code): Assign “Y” if all conditions represented by the single ICD-10-CM code were present on admission (e.g. bilateral unspecified age-related cataracts).
When to use counseling Z codes?
Counseling Z codes are used when a patient or family member receives assistance in the aftermath of an illness or injury, or when support is required in coping with family or social problems.
When assigning a chapter 15 code for sepsis complicating abortion, pregnancy, childbirth, and the?
When assigning a chapter 15 code for sepsis complicating abortion, pregnancy, childbirth, and the puerperium, a code for the specific type of infection should be assigned as an additional diagnosis. If severe sepsis is present, a code from subcategory R65.2, Severe sepsis, and code(s) for associated organ dysfunction(s) should also be assigned as additional diagnoses.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion '), unless the combination is specifically indexed elsewhere. For multiple neoplasms of the same site that are not contiguous such as tumors in different quadrants of the same breast, codes for each site should be assigned.
What is the Z85 code for a primary malignancy?
When a primary malignancy has been previously excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy at that site, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy. Any mention of extension, invasion, or metastasis to another site is coded as a secondary malignant neoplasm to that site. The secondary site may be the principal or first-listed with the Z85 code used as a secondary code.
How to reference neoplasm table?
The neoplasm table in the Alphabetic Index should be referenced first. However, if the histological term is documented, that term should be referenced first, rather than going immediately to the Neoplasm Table, in order to determine which column in the Neoplasm Table is appropriate. Alphabetic Index to review the entries under this term and the instructional note to “see also neoplasm, by site, benign.” The table provides the proper code based on the type of neoplasm and the site. It is important to select the proper column in the table that corresponds to the type of neoplasm. The Tabular List should then be referenced to verify that the correct code has been selected from the table and that a more specific site code does not exist.
What is Chapter 2 of the ICD-10-CM?
Chapter 2 of the ICD-10-CM contains the codes for most benign and all malignant neoplasms. Certain benign neoplasms , such as prostatic adenomas, may be found in the specific body system chapters. To properly code a neoplasm, it is necessary to determine from the record if the neoplasm is benign, in-situ, malignant, or of uncertain histologic behavior. If malignant, any secondary ( metastatic) sites should also be determined.
When a pregnant woman has a malignant neoplasm, should a code from subcatego?
When a pregnant woman has a malignant neoplasm, a code from subcategory O9A.1 -, malignant neoplasm complicating pregnancy, childbirth, and the puerperium, should be sequenced first, followed by the appropriate code from Chapter 2 to indicate the type of neoplasm. Encounter for complication associated with a neoplasm.
When is the primary malignancy or appropriate metastatic site designated as the principal or first-listed diagnosis?
When the reason for admission/encounter is to determine the extent of the malignancy, or for a procedure such as paracentesis or thoracentesis, the primary malignancy or appropriate metastatic site is designated as the principal or first-listed diagnosis, even though chemotherapy or radiotherapy is administered.
When a patient is admitted because of a primary neoplasm with metastasis and treatment is?
When a patient is admitted because of a primary neoplasm with metastasis and treatment is directed toward the secondary site only , the secondary neoplasm is designated as the principal diagnosis even though the primary malignancy is still present .
What is C649 in kidney?
for glandular (adeno) carcinoma of the kidney. Approximately 85% of all malignancies of the kidney C649 are RCC or subtypes/variants of RCC.
When was the WHO classification of tumors of the Urinary System and Male Genital Organs published?
These changes are effective with cases diagnosed 1/1/2018 and later. WHO Classification of Tumors of the Urinary System and Male Genital Organs was published in 2016.
Is renal cell carcinoma the same as leiomyomatosis?
Hereditary leiomyomatosis and renal cell carcinoma- associated renal cell carcinoma , MiT family translocation renal cell carcinomas , and succinate dehydrogenase-deficient renal cell carcinomas have the same ICD-O code but are distinctly different histologies. Because they are different, they are on different lines in column 3 (see M rules) .
Is sarcomatoid carcinoma a specific subtype?
WHO, IARC, and CAP agree that sarcomatoid carcinoma is a pattern of differentiation, not a specific subtype, of renal cell carcinoma.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
When will the ICd 10 C64.1 be released?
The 2022 edition of ICD-10-CM C64.1 became effective on October 1, 2021.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What is the code for adenocarcinoma?
Diagnosis for a single tumor is adenocarcinoma 8140 with the majority or predominant part of tumor being enteric- type adenocarcinoma 8144. Code the subtype/variant: enteric-type adenocarcinoma 8144. Example 2:
Is a benign CNS tumor grade 1 or grade 2?
For the most part, benign CNS tumors (/0) and uncertain if benign or malignant CNS tumors (/1) are WHO Grade I. They may be given a WHO Grade II based on histologic features, clinical findings, and genetic testing. Grade II CNS tumors tend to be slow growing but may spread into nearby tissue or recur.
Popular Posts:
- 1. icd 10 code screening for ultrasound
- 2. icd 10 code for left breast mass at 11 o'clock
- 3. icd-10 code for personal history of lipoma
- 4. icd 10 code for cardiorespiratory failure
- 5. icd 10 code for t3 uptake test
- 6. icd 10 diagnosis code for hemodialysis
- 7. icd-10 code for right wrist tendonitis
- 8. icd 10 code for cyst right thumb
- 9. icd 10 code for benign lichenoid keratosis
- 10. 2021 icd 10 code for chronic low back pain