Respiratory failure, not elsewhere classified. J96 should not be used for reimbursement purposes as there are multiple codes below it that contain a greater level of detail. The 2019 edition of ICD-10-CM J96 became effective on October 1, 2018. This is the American ICD-10-CM version of J96 - other international versions of ICD-10 J96 may differ.
J96 Respiratory failure, not elsewhere classified
syndrome of adult (J80)What are the new ICD 10 codes?
The new codes are for describing the infusion of tixagevimab and cilgavimab monoclonal antibody (code XW023X7), and the infusion of other new technology monoclonal antibody (code XW023Y7).
Where can one find ICD 10 diagnosis codes?
Search the full ICD-10 catalog by:
- Code
- Code Descriptions
- Clinical Terms or Synonyms
What are ICD 10 codes?
Why ICD-10 codes are important
- The ICD-10 code system offers accurate and up-to-date procedure codes to improve health care cost and ensure fair reimbursement policies. ...
- ICD-10-CM has been adopted internationally to facilitate implementation of quality health care as well as its comparison on a global scale.
- Compared to the previous version (i.e. ...
What is the ICD 10 diagnosis code for?
The ICD-10-CM is a catalog of diagnosis codes used by medical professionals for medical coding and reporting in health care settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates.
What is the ICD-10 DX code for respiratory failure?
ICD-10 code J96. 90 for Respiratory failure, unspecified, unspecified whether with hypoxia or hypercapnia is a medical classification as listed by WHO under the range - Diseases of the respiratory system .
How do you code respiratory failure?
Acute Respiratory Failure as Principal Diagnosis A code from subcategory J96. 0, Acute respiratory failure, or subcategory J96. 2, Acute and chronic respiratory failure, may be assigned as a principal diagnosis when it is the condition established after study to be chiefly responsible for the hospital admission.
What are the 4 types of respiratory failure?
Classification:Type 1 (Hypoxemic ) - PO2 < 50 mmHg on room air. Usually seen in patients with acute pulmonary edema or acute lung injury. ... Type 2 (Hypercapnic/ Ventilatory ) - PCO2 > 50 mmHg (if not a chronic CO2 retainer). ... Type 3 (Peri-operative). ... Type 4 (Shock) - secondary to cardiovascular instability.
What is the ICD-10-CM code for hypoxic respiratory failure?
01.
When do you code chronic respiratory failure?
In ICD-10-CM the classification of Respiratory Failure (J96) includes “acute (J96. 0-)”, “chronic” (J96. 1-). “acute and chronic” (J96.
Can respiratory failure be principal diagnosis?
So, acute respiratory failure can be coded if the condition meets the definition for the principal diagnosis and is clinically supported in the medical record by a hands-on treating provider without any conflict existing in the documentation between any consulting and attending provider.
What is the difference between Type 1 and 2 respiratory failure?
Respiratory failure is divided into type I and type II. Type I respiratory failure involves low oxygen, and normal or low carbon dioxide levels. Type II respiratory failure involves low oxygen, with high carbon dioxide.
Is COPD type 1 or type 2 respiratory failure?
Preventing Type 1 and Type 2 Respiratory Failure Causes of type 1 respiratory failure include: pulmonary oedema, pneumonia, COPD, asthma, acute respiratory distress syndrome, chronic pulmonary fibrosis, pneumothorax, pulmonary embolism, pulmonary hypertension.
Is COPD type 2 respiratory failure?
Type II respiratory failure involves low oxygen, with high carbon dioxide (pump failure). It occurs when alveolar ventilation is insufficient to excrete the carbon dioxide being produced. The most common cause is chronic obstructive pulmonary disease (COPD).
Is respiratory insufficiency the same as respiratory failure?
Respiratory insufficiency and failure can be defined broadly as the impairment of respiratory gas exchange between the ambient air and circulating blood. Respiratory insufficiency and failure are generally categorized into one of two types—hypercapnic or hypoxemic.
What is Hypoxemic respiratory failure?
Hypoxemic respiratory failure means that you don't have enough oxygen in your blood, but your levels of carbon dioxide are close to normal. Hypercapnic respiratory failure means that there's too much carbon dioxide in your blood, and near normal or not enough oxygen in your blood.
What is Acute respiratory failure with hypoxia?
ARF occurs when the respiratory system is unable to either adequately absorb oxygen (i.e., hypoxemia) or excrete carbon dioxide (i.e., hypercarbia). Although both hypoxemia and hypercarbia can occur together, one process frequently predominates.
What is the ICd 10 code for respiratory failure?
Respiratory failure, unspecified with hypoxia 1 J96.91 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. 2 The 2021 edition of ICD-10-CM J96.91 became effective on October 1, 2020. 3 This is the American ICD-10-CM version of J96.91 - other international versions of ICD-10 J96.91 may differ.
When will the ICd 10 J96.91 be released?
The 2022 edition of ICD-10-CM J96.91 became effective on October 1, 2021.
What is the CPT code for respiratory impairment?
Therapeutic procedures whose principle aim is to treat a respiratory impairment should be identified using the G0237-G0239 series of HCPCS codes. CPT® codes 97000 to 97799 are not to be billed by professionals involved in treating respiratory conditions, unless these services are delivered by physical or occupational therapists and meet the other requirements for physical and occupational therapy services.
Why do contractors need to specify revenue codes?
Contractors may specify Revenue Codes to help providers identify those Revenue Codes typically used to report this service. In most instances Revenue Codes are purely advisory. Unless specified in the article, services reported under other Revenue Codes are equally subject to this coverage determination. Complete absence of all Revenue Codes indicates that coverage is not influenced by Revenue Code and the article should be assumed to apply equally to all Revenue Codes.
Is CPT a year 2000?
CPT is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to, the implied warranties of merchantability and fitness for a particular purpose. AMA warrants that due to the nature of CPT, it does not manipulate or process dates, therefore there is no Year 2000 issue with CPT. AMA disclaims responsibility for any errors in CPT that may arise as a result of CPT being used in conjunction with any software and/or hardware system that is not Year 2000 compliant. No fee schedules, basic unit, relative values or related listings are included in CPT. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this file/product is with CMS and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this file/product. This Agreement will terminate upon no upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
What are the symptoms of respiratory failure?
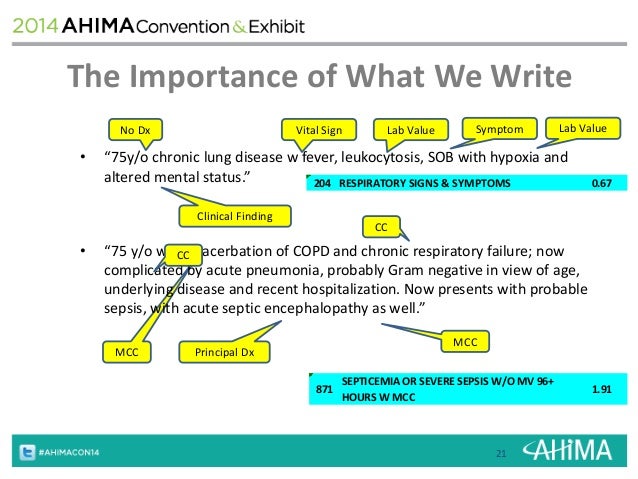
Look for documented signs / symptoms of: SOB (shortness of breath) Delirium and/or anxiety. Syncope. Use of accessory muscles / poor air movement.
When is acute respiratory failure a principal diagnosis?
OFFICIAL CODING GUIDELINE Acute or acute on chronic respiratory failure may be reported as principal diagnosis when it is the condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care. Refer to Section II of the ICD-10-CM Official Guidelines for Coding and Reporting on “Selection of Principal Diagnosis”.
What to do if documentation is not clear as to whether acute respiratory failure and another condition are equally responsible for occasioning?
If the documentation is not clear as to whether Acute Respiratory Failure and another condition are equally responsible for occasioning the admission, query the provider for clarification.
Is respiratory failure a cut and dry diagnosis?
Very seldom is it a simple cut and dry diagnosis. There always seems to be just enough gray to give coders on any given day some doubt. It’s not only important for a coder to be familiar with the guidelines associated with respiratory failure but they should also be aware of the basic clinical indicators as well.
Can COPD cause ABG?
A patient with a chronic lung disease such as COPD may have an abnormal ABG level that could actually be considered that particular patient’s baseline.
What is respiratory failure?
Respiratory failure, not elsewhere classified. Clinical Information. Life-threatening respiratory failure that develops rapidly. Causes include injury, sepsis, drug overdose, and pancreatitis. It manifests with dyspnea and cyanosis and may lead to cardiovascular shock.
When will the ICD-10 J96.0 be released?
The 2022 edition of ICD-10-CM J96.0 became effective on October 1, 2021.
What are the symptoms of respiratory failure?
Signs and symptoms of respiratory failure may include shortness of breath, rapid breathing, and air hunger (feeling like you can not breathe in enough air).
Is respiratory failure a secondary diagnosis?
Secondary diagnosis: Respiratory failure may be listed as a secondary diagnosis if it occurs after admission, or if it is present on admission, but does not meet the definition of principal diagnosis.
Is supplemental oxygen an acute exacerbation?
Worsening of symptoms requiring an increase in supplemental oxygen also indicates an “acute exacerbation” of chronic respiratory failure.
Popular Posts:
- 1. icd 10 code for blood blister 3rd left toe
- 2. icd 9 code for graves disease
- 3. icd 10 code for 311
- 4. icd 10 code for compound fracture, type ii, left shaft of tibia
- 5. icd 1o code for left temporal lobe bone fracture
- 6. icd 10 code for percutaneous electrosurgical ablation of a lesion of the right diaphragm
- 7. icd 10 code for cervical lymphadenopathy
- 8. icd 10 code for abnormal murmur
- 9. icd 10 cm code for toenail avulsion
- 10. icd 10 code for makena injection