Femoroacetabular Impingement ICD-10 M25.851 - Other specified joint disorders, right hip M25.852 - Other specified joint disorders, left hip
Femoroacetabular Impingement ICD-10
- M25.851 - Other specified joint disorders, right hip.
- M25.852 - Other specified joint disorders, left hip.
- M25.859 - Other specified joint disorders, unspecified hip.
- M25.551 - Pain in right hip.
- M25.552 - Pain in left hip.
- M25.559 - Pain in unspecified hip.
What is femoroacetabular impingement?
Femoroacetabular Impingement Femoroacetabular impingement (FAI) is a condition in which extra bone grows along one or both of the bones that form the hip joint — giving the bones an irregular shape. Because they do not fit together perfectly, the bones rub against each other during movement.
What is the ICD 10 code for impingement syndrome of the shoulder?
ICD-10-CM Diagnosis Code M75.40 [convert to ICD-9-CM] Impingement syndrome of unspecified shoulder Impingement syndrome of shoulder; Impingement syndrome of shoulder region
What is the ICD 10 code for hip fracture?
M25.859 is a valid billable ICD-10 diagnosis code for Other specified joint disorders, unspecified hip . It is found in the 2021 version of the ICD-10 Clinical Modification (CM) and can be used in all HIPAA-covered transactions from Oct 01, 2020 - Sep 30, 2021 .
How is femoroacetabular impingement syndrome (FIP) treated?
Arthroscopic Surgery or Physical Therapy for Patients With Femoroacetabular Impingement Syndrome: A Randomized Controlled Trial With 2-Year Follow-up. Am J Sports Med. 2018 Feb 1:363546517751912. doi: 10.1177/0363546517751912.
What is the ICD-10 code for femoroacetabular impingement?
851.
What is femoroacetabular impingement?
Hip impingement, or femoroacetabular impingement (FAI), occurs when the femoral head (ball of the hip) pinches up against the acetabulum (cup of the hip). When this happens, damage to the labrum (cartilage that surrounds the acetabulum) can occur, causing hip stiffness and pain, and can lead to arthritis.
What are the two types of femoroacetabular impingement?
There are three types of FAI: pincer, cam, and combined impingement.
Is femoroacetabular impingement the same as hip dysplasia?
Impingement is not usually caused by dysplasia, but it can be painful. The pain is more like a pinching pain in certain positions of sitting or hip movement like a high kick when dancing. Impingement is usually caused by an abnormal shape of the neck of the femur just below the head.
Is femoroacetabular impingement a disease?
Femoroacetabular impingement (FAI), also called hip impingement, is a condition where the hip joint is not shaped normally. This causes the bones to painfully rub together. This condition can be treated with corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, rest and surgery.
Is femoroacetabular impingement common?
FAI is a common, often unrecognised condition causing hip pain and degenerative hip disease.
What causes hip femoroacetabular impingement?
Hip impingement may be caused by a misshapen femoral head, deformed femoral neck, or a hip socket that covers too much of the femoral head. Over time, repetitive “bumping” or impingement of the femur on the rim of the acetabulum leads to cartilage and labral damage.
What is the best treatment for hip impingement?
If hip impingement syndrome causes aching pain and limits your ability to move without discomfort, your doctor may recommend an over-the-counter pain relief medication. Many doctors recommend acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs), which include aspirin, ibuprofen, and naproxen.
Does hip impingement lead to hip replacement?
Hip impingement causes friction and abnormal wear and tear on the joint. Overtime, this can lead to osteoarthritis and the need for a hip replacement.
Does femoroacetabular impingement require surgery?
If hip impingement syndrome causes significant pain and symptoms don't improve with nonsurgical treatment or therapeutic injections, our orthopedic surgeons may recommend surgery. They can reshape the bones in the hip joint, so that the round femoral head can rotate smoothly within the socket-shaped acetabulum.
What is cam type femoroacetabular impingement of the hip?
Cam-type femoroacetabular impingement (FAI) is a known cause of groin pain and a condition that can give rise to osteoarthritis of the hip (1). Patients suffering from this condition are mainly young and experience pain when the hip is moved through internal rotation and adduction at 90° of hip flexion.
Can you have hip dysplasia and FAI?
Bony abnormalities associated with acetabular dysplasia (AD) and femoroacetabular impingement (FAI) have been recently implicated as risk factors for hip osteoarthritis (OA).
How do you fix femoroacetabular impingement?
Treatment for hip impingement should begin with: Resting the affected hip. Modifying your activities to avoid moving the joint in a way that causes pain. Exercising as recommended by your doctor or physical therapist to strengthen the muscles that support the hip.
Does femoroacetabular impingement go away?
However, most patients will make a full recovery in four to six months. Many instances of FAI can be adequately managed with a personalized approach to conservative care treatment.
What does femoroacetabular impingement feel like?
Symptoms initially include pain in your groin and a decreased range of motion of your hip. At first, you might only feel pain when the motion of your hip nears its limits, but as the condition worsens, you may start to feel pain during normal activities like walking uphill.
What does femoral acetabular impingement feel like?
Symptoms include a dull, aching pain in the groin that may get worse during movement and exercise, the sensation or sound of clicking or popping in the hip joint during movement, and stiffness in the thigh, hip, or groin.
What is the condition of hip impingement?
Hip impingement syndrome, also known as femoro-acetabular impingement (FAI) syndrome, is a recently accepted pathological condition that primarily affects young and middle-aged adults. It is characterized by hip pain felt mainly in the groin, and can result in chronic pain and decreased range of motion in flexion and internal rotation. Femoroacetabular impingement (FAI) occurs as a result of friction in the hip joint caused by abnormal contact between the femoral head and the rim of the acetabulum (hip socket). Over time, the repetitive contact can cause damage to the articular or labral cartilage, which may lead to degenerative joint disease.
What is cam impingement?
Cam Impingement is a type of impingement in which the femoral head is aspherical, which prevents it from rotating smoothly inside the acetabulum (i.e., femoral cause ). Pincer Impingement is a type of impingement in which extra bone extends out over the normal rim of the acetabulum (ie, acetabular cause).
Why is hip arthroscopy considered experimental and investigational?
Aetna considers hip arthroscopy to repair degenerative labral tears (e.g., due to early osteoarthritis) experimental and investigational. Aetna considers labrum reconstruction experimental and investigational for the treatment of FAI because there is insufficient evidence regarding the effectiveness of this approach.
Is femoro acetabular surgery considered a medical procedure?
Aetna considers femoro-acetabular surgery, open or arthroscopic, for the treatment of hip impingement syndrome medically necessary for persons who fulfil all the following criteria:
Is femoro acetabular impingement a progressive condition?
Femoro-acetabular impingement syndrome has been reported to be associated with progressive osteoarthritis of the hip. History, physical examination, as well as supportive radiographical findings including evidence of articular cartilage damage, acetabular labral tearing, and early-onset degenerative changes can aid in diagnosing this condition. Several pathological changes of the femur and acetabulum are known to predispose individuals to develop FAI syndrome.
Why is femoral shaving coded separately?
The femoral shaving is coded separately because it is a procedure performed on the femur rather than on the hip joint. The capsulotomy and synovectomy were performed to access the procedure site and are not coded separately. Assign the ICD-10-PCS codes as follows:
What is the code for a labral tear?
Assign code S73.192A, Other sprain of left hip, initial encounter, for the labral tear. Assign code M25.852, Other specified joint disorders, left hip, for the femoroacetabular impingement.
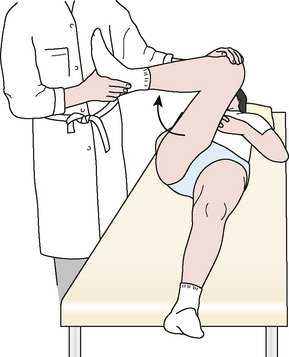
How to know if you have an impingement?
As part of the physical examination, your doctor will likely conduct the impingement test. For this test, your doctor will bring your knee up towards your chest and then rotate it inward towards your opposite shoulder. If this recreates your hip pain, the test result is positive for impingement.
Which part of the hip fits perfectly into the acetabulum?
In a healthy hip, the femoral head fits perfectly into the acetabulum.
What to do if your hip is aching?
The longer painful symptoms go untreated, the more damage FAI can cause in the hip.
What is the joint between the hip and the socket?
Anatomy. The hip is a ball-and-socket joint. The socket is formed by the acetabulum, which is part of the large pelvis bone. The ball is the femoral head, which is the upper end of the femur (thighbone). A slippery tissue called articular cartilage covers the surface of the ball and the socket.
How to help hip pain?
Sometimes, you can modify your activities, let your hip rest, and see if the pain will settle down. Over-the-counter anti-inflammatory medicines, such as ibuprofen and naproxen, may help.
Can surgery fix hip impingement?
However, not all of the damage can be completely fixed by surgery, especially if treatment has been put off and the damage is severe.
What is slipped capital femoral epiphysis?
History of childhood hip disease (e.g. slipped capital femoral epiphysis (SCFE) or Legge-Calve-Perthes disease) which may have altered the shape of the femoral head. Malunion following femoral neck fractures which may have altered the contour of the femoral head/neck.
What is the hip joint?
The hip (acetabulofemoral joint) is a synovial joint formed between the femur and acetabulum of the pelvis. The head of the femur is covered by Type II collagen (hyaline cartilage) and proteoglycan. The acetabulum is the concave portion of the ball and socket joint.
How to improve hip function?
To improve dynamic stability of the hip, there should be a focus on strengthening the deep hip external rotators, abductors and flexors in the transverse, frontal and sagittal planes. With this approach, the authors propose that for at least some patients with symptomatic FAI, loading of the labrum could be reduced which would then facilitate downregulation of nociceptive neurotransmitters in the labrum. As well, strengthening could help with more generalized inflammation in the hip joint that is commong with FAI syndrome.
Does wearing a brace affect hip impingement?
Newcomb et al (2018) investigated the immediate and longer term effects of wearing a brace (a Don Joy S.E.R.F./Stability through External Rotation of the Femur model). They found that the brace did modify the kinematics of patients with FAI by limiting movements that were associated with hip impingement (flexion, internal rotation and adduction of the hip) during common activities (squat, stair climbing and stair descending). The single limb squat was also studied but the brace did not change the kinematics involved with this task. The kinematic changes that were identified did not, however, lead to decreased pain or improvement in patient-reported outcomes either immediately or after four weeks of daily brace use. The authors' conclusion was that there may be a sub-group of patients with FAI syndrome that may benefit from bracing but based on their particular study, the use of bracing is not supported as a general conservative therapy for this condition.

Popular Posts:
- 1. icd 10 cm code for interaction of codine
- 2. icd 10 code for blood loss after surgery
- 3. blood work for std screen icd code
- 4. icd 10 code for right knee instability
- 5. icd code for recurrent otitis media
- 6. icd 9 code for labral tear of right shoulder
- 7. 2019 icd 10 code for breast ultrasound post op due to implants
- 8. icd 10 code for right breast diagnostic sonogram and mammogram
- 9. icd 10 code for abrasions to lower legs
- 10. icd 10 code for er positive