Congenital dilation of aorta
Q25. 44 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Q25. 44 became effective on October 1, 2021.How is a dilated aortic root repaired?
Valve sparing surgery becomes very much essential to cure the enlarged aortic root or its aneurysm. Surgeons thus remove the enlarged section and replace them with the synthetic tube referred as graft. During the surgical procedure, doctors keep the aortic valve of a patient aside and use it again.
What causes a mildly ectatic aorta?
A Guide to the Causes, Signs and Symptoms, and Available Treatments
- About. Mild aortic ectasia is defined as an enlargement of the aorta that is mild in degree. ...
- Risk of Rupture. Though the term ‘mild’ may indicate a lack in the seriousness of the condition, aortic aneurysms are serious.
- Echocardiography. ...
- Other Factors. ...
- Symptoms. ...
- Treatment. ...
- Summary. ...
- References. ...
What is treatment for enlarged aortic root?
With our minimally invasive aortic root valve replacement procedure, patients can generally expect:
- Shorter hospital stay
- Less post-surgical pain due to a smaller incision, better chest wall stability, and no broken sternum
- Less blood loss during surgery
- Less downtime and restrictions – our patients can resume normal exercise, daily movement, driving, and work in a few weeks compared to several months with traditional open-heart surgery
What is root dilatation of the aorta?
Comments
- The left ventricular chamber size is normal. There is normal left
- There is trivial mitral and mild tricuspid regurgitation.
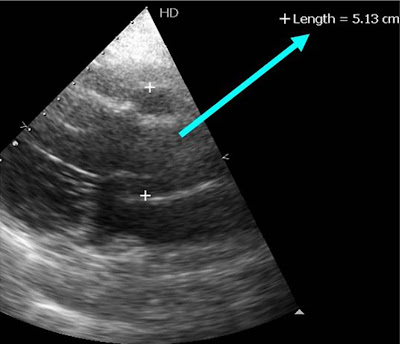
- There is severe dilatation of the ascending aorta 5.0 cm
- The aortic valve appears bicuspid. There is mild aortic stenosis. The

What is aortic root dilatation?
Otherwise known as an aortic root aneurysm, a dilated aortic root is when the first section of the aorta, where the aortic valve resides, becomes enlarged. When this enlargement reaches a critical size, there is a risk of it rupturing or tearing, leading to a life-threatening situation.
Is the aortic root part of the thoracic aorta?
The Thoracic Aorta has 4 distinct parts: Aortic Root – Lies in the front portion of the chest below the sternum. It starts at the level of the heart and includes the aortic valve and the portion where the coronary arteries arise called the Sinus of Valsalva.
Where is aortic root located?
The aorta is the large blood vessel that carries blood from the heart to the body. The aortic root is located near where the aorta and the heart connect.
Is aortic root ascending or descending?
The ascending aorta originates beyond the aortic valve and ends right before the innominate artery (brachiocephalic trunc). It is approximately 5 cm long and is composed of two distinct segments. The lower segment, known as the aortic root, encompasses the sinuses of Valsalva and sinotubular junction (STJ).
What causes a dilated aortic root?
Progressive dilatation of the aortic root is caused by medial degeneration and destruction of the elastic and collagen fibers and can be also associated with high blood pressure, high stroke volume, and inflammatory diseases [14–17].
How is a dilated aortic root treated?
Aortic root surgery. This type of open-chest surgery is done to treat an enlarged section of the aorta to prevent a rupture. Aortic aneurysms near the aortic root may be related to Marfan syndrome and other related condition. A surgeon removes part of the aorta and sometimes the aortic valve.
Is aortic root the same as aortic valve?
The term 'aortic root' refers to the aortic valve from its position at the left ventricular outlet to its junction with the ascending portion of the aorta. Anatomically, this whole structure is the aortic valve. The normal aortic valve is more complex than its three semilunar leaflets suggests.
What is dilated aortic root and ascending aorta?
An ascending aortic aneurysm is a weak spot in the top part of your aorta, which is the main artery in your body. The aneurysm bulges outward, and may cause your blood vessel wall to tear or break open. It's a life-threatening condition.
Is a dilated aortic root common?
Dilated aortic root (DAR) is a relatively common finding, with a reported prevalence of about 4% measured at the level of the sinuses of Valsalva in the general population.
What size is a dilated aortic root?
Dilation of the aortic root imparts a significant higher risk of adverse events. A diameter shift for intervention to 5.0 cm for the aortic root and to 5.25 cm for the mid‐ascending aorta should be considered at expert centers.
What are the branches of thoracic aorta?
The major noncoronary branches of the thoracic aorta are (in order) the innominate (also known as the brachiocephalic) artery, the left common carotid artery, and the left subclavian artery. The innominate artery bifurcates into the right common carotid and right subclavian arteries.
What is thoracic aorta?
The aorta is the largest artery in the body and is the blood vessel that carries oxygen-rich blood away from the heart to all parts of the body. The section of the aorta that runs through the chest is called the thoracic aorta and, as the aorta moves down through the abdomen it is called the abdominal aorta.
What are the branches of the aorta?
The convexity of the aortic arch gives off three branches; the brachiocephalic trunk, the left common carotid artery and the left subclavian artery.
Where does the thoracic aorta end?
The descending thoracic aorta begins at the lower border of the fourth thoracic vertebra and ends in front of the lower border of the twelfth thoracic vertebra, at the aortic hiatus in the diaphragm where it becomes the abdominal aorta.
Open Approach
Cutting through the skin or mucous membrane and any other body layers necessary to expose the site of the procedure
Percutaneous Approach
Entry, by puncture or minor incision, of instrumentation through the skin or mucous membrane and any other body layers necessary to reach the site of the procedure
Percutaneous Endoscopic Approach
Entry, by puncture or minor incision, of instrumentation through the skin or mucous membrane and any other body layers necessary to reach and visualize the site of the procedure
Popular Posts:
- 1. icd 10 code for tobacco use in remission
- 2. icd-10-cm code for hidradenitis suppurative bilateral axilla
- 3. icd-10-cm code for rsv
- 4. icd code for minimal brain dysfuntions
- 5. icd 10 code for admit b12 injection
- 6. icd 10 cm code for concentric left ventricular hypertrophy.
- 7. icd 10 code for acute pain trauma
- 8. icd 10 code for anaphlatic shock allergy to bee sting
- 9. icd 10 cm code for right thumb sprain
- 10. icd-10 code for right fingernail pain hx of trauma