1 for Chronic obstructive pulmonary disease with (acute) exacerbation is a medical classification as listed by WHO under the range - Diseases of the respiratory system .
Full
AnswerWhat is the diagnosis code for COPD?
The ICD code J44 is used to code Chronic obstructive pulmonary disease Chronic obstructive pulmonary disease (COPD), also known as chronic obstructive lung disease (COLD) and chronic obstructive airway disease (COAD), among others, is a type of obstructive lung disease characterized by chronically poor airflow. It typically worsens over time.
What are the guidelines for COPD?
These supplement the existing recommendations on:
- diagnosing COPD using symptoms, spirometry and other tests
- managing stable COPD using nebulisers, oral therapy and pulmonary rehabilitation
- multidisciplinary management of stable COPD, including physiotherapy, occupational therapy, nutrition and palliative care
- managing exacerbations of COPD in primary care and in hospital
What is the diagnosis for COPD?
Tests may include:
- Lung (pulmonary) function tests. These tests measure the amount of air you can inhale and exhale, and whether your lungs deliver enough oxygen to your blood. ...
- Chest X-ray. A chest X-ray can show emphysema, one of the main causes of COPD. ...
- CT scan. ...
- Arterial blood gas analysis. ...
- Laboratory tests. ...
What is the J code for COPD?
chronic obstructive pulmonary disease [COPD] with acute bronchitis ICD-10-CM Diagnosis Code J44.0 Chronic obstructive pulmonary disease with (acute) lower respiratory infection

What is the ICD-10 code for COPD with exacerbation?
ICD-10 code: J44. 1 Chronic obstructive pulmonary disease with acute exacerbation, unspecified.
What is the ICD-10-CM code for COPD?
ICD-Code J44. 9 is a billable ICD-10 code used for healthcare diagnosis reimbursement of Chronic obstructive pulmonary disease. This is sometimes referred to as chronic obstructive lung disease (COLD) or chronic obstructive airway disease (COAD).
How do you code a COPD exacerbation?
The Alphabetic Index leads coding professionals to code J44. 1, COPD with (acute) exacerbation, for exacerbation of COPD.
What is the ICD-10 code for exacerbation?
ICD-10-CM Code for Unspecified asthma with (acute) exacerbation J45. 901.
What is acute exacerbation of COPD?
An acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a clinical diagnosis made when a patient with COPD experiences a sustained (e.g., 24–48 h) increase in cough, sputum production, and/or dyspnea.
What is a COPD exacerbation?
Exacerbations of chronic obstructive pulmonary disease (COPD) are episodes of worsening of symptoms, leading to substantial morbidity and mortality. COPD exacerbations are associated with increased airway and systemic inflammation and physiological changes, especially the development of hyperinflation.
What is the ICD 10 code for COPD exacerbation with emphysema?
The Alphabetic Index leads coding professionals to code J44. 1, COPD with (acute) exacerbation, for exacerbation of COPD. However, Coding Clinic Fourth Quarter 2017 advises to assign code J43. 9, Emphysema, unspecified, when a patient with emphysema presents with an acute exacerbation of COPD.
Can J44 0 and J44 1 be coded together?
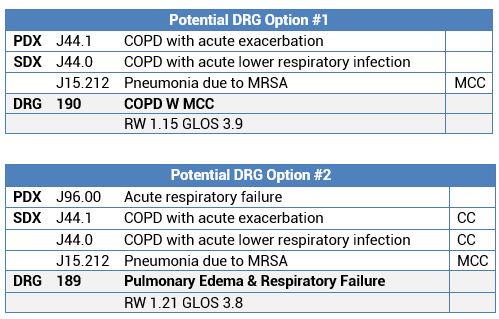
0 is coded first, followed by the code for pneumonia, and assigned to DRG 190 COPD with MCC. AECOPD and Pneumonia: When a patient has both pneumonia and acute exacerbation of COPD, it is appropriate to assign both codes J44. 0 [COPD with acute lower respiratory infection] and J44. 1 [COPD with (acute) exacerbation].
What is the diagnosis for ICD-10 code r50 9?
9: Fever, unspecified.
Why is COPD difficult to code?
Since the term COPD is unspecified and represents any form of unspecified chronic obstructive lung disease, an additional code is not needed when the diagnosis of emphysema is documented in the healthcare record. The emphysema is the specified type of COPD.
Can you code both asthma and COPD together?
If the documentation supports that the patient has a specific type of asthma documented and COPD, both codes could be reported. An example would be documentation in the record is COPD and moderate persistent asthma.
Is bronchitis a COPD exacerbation?
Chronic bronchitis (CB) is closely associated with the frequency and severity of chronic obstructive pulmonary disease (COPD) exacerbation. However, little is known about the impact of CB on COPD exacerbations, severe and non-severe, and on recovery from an exacerbation.
Do you code both COPD and emphysema?
So if documentation shows a patient with emphysema presents due to asthma and COPD, HCPCS Coding Clinic® (vol. 6, no. 1), instructs you to report J43. 9 for the emphysema and a code from J45.
What is the ICd 10 code for COPD?
COPD ICD 10 codes and guidelines can be found in chapter 10 of ICD-10-CM manual which is “diseases of the respiratory system”, code range J00 – J99
What are the codes for COPD?
COPD ICD 10 Code list and guidelines 1 As COPD is a group of diseases it is important to see the coding guidelines properly before deciding which code to be assigned. 2 Look for the notes – Excludes 1, excludes 2, includes, code also, use additional. 3 Excludes 1 note has codes from category J43, J41, J42, J47 and J68.0 4 Asthma of specified type (Eg: mild intermittent asthma) should be coded separately along with COPD. 5 Disease – Airway – Obstructive = Leads to COPD
What are the most common causes of COPD?
Groups of lung diseases contribute to COPD, most commonly seen combinations are Emphysema and chronic bronchitis. Cigarette smoking is one of the major risk factor in increasing the number of COPD patients in the world.
How to diagnose COPD?
Diagnosis of COPD can be done by doing pulmonary function test (PFT), chest X-ray, CT lung or arterial blood gas analysis.
Can J45.909 be coded with COPD?
Note: asthma unspecified J45.909 can not be coded with COPD. Asthma can be coded only if it is specified to which type.
Can you code J43.9?
Can not code J43.9 (emphysema) as it has excludes 1 note for “emphysema with chronic (obstructive) bronchitis (J44.-)
Is COPD a group disease?
As COPD is a group of diseases it is important to see the coding guidelines properly before deciding which code to be assigned.
What is a COPD?
A disease of chronic diffuse irreversible airflow obstruction. Subcategories of copd include chronic bronchitis and pulmonary emphysema.
What are the symptoms of chronic obstructive pulmonary disease?
Signs and symptoms include shortness of breath, wheezing, productive cough, and chest tightness. The two main types of chronic obstructive pulmonary disease are chronic obstructive bronchitis and emphysema. A disease of chronic diffuse irreversible airflow obstruction. Subcategories of copd include chronic bronchitis and pulmonary emphysema.
What is a chronic lung disorder?
A chronic and progressive lung disorder characterized by the loss of elasticity of the bronchial tree and the air sacs, destruction of the air sacs wall, thickening of the bronchial wall, and mucous accumulation in the bronchial tree.
What is the name of the disease that causes the alveoli to be damaged?
Chronic obstructive pulmonary disease includes chronic bronchitis, in which the bronchi (large air passages) are inflamed and scarred, and emphysema, in which the alveoli (tiny air sacs) are damaged. It develops over many years and is usually caused by cigarette smoking.
When will the ICD-10 J44.9 be released?
The 2022 edition of ICD-10-CM J44.9 became effective on October 1, 2021.
What causes a person to breathe hard?
Chronic obstructive pulmonary disease (copd) makes it hard for you to breathe. Coughing up mucus is often the first sign of copd. Chronic bronchitis and emphysema are common copds. Your airways branch out inside your lungs like an upside-down tree. At the end of each branch are small, balloon-like air sacs. In healthy people, both the airways and air sacs are springy and elastic. When you breathe in, each air sac fills with air like a small balloon. The balloon deflates when you exhale. In copd, your airways and air sacs lose their shape and become floppy, like a stretched-out rubber band.cigarette smoking is the most common cause of copd. Breathing in other kinds of irritants, like pollution, dust or chemicals, may also cause or contribute to copd. quitting smoking is the best way to avoid developing copd. Treatment can make you more comfortable, but there is no cure.
What is the ICd 10 code for COPD?
ICD-10-CM 2020 is bringing a small change to chronic obstructive pulmonary disease (COPD) code J44.0, making it a good time to refresh your knowledge of the guidelines that apply to coding for this disease (or group of diseases, if you want to be precise!).
What is the code for acute exacerbation of chronic obstructive bronchitis?
Acute exacerbation of chronic obstructive bronchitis and asthma#N#The codes in categories J44 and J45 distinguish between uncomplicated cases and those in acute exacerbation. An acute exacerbation is a worsening or a decompensation of a chronic condition. An acute exacerbation is not equivalent to an infection superimposed on a chronic condition, though an exacerbation may be triggered by an infection.
How to avoid COPD coding mistakes?
To avoid COPD coding mistakes, you must apply the notes that accompany the codes in the ICD-10-CM Tabular List. Payers are increasingly paying attention to whether claims follow Excludes1 notes, so your ability to follow the notes may help prevent denials.
What is parentheses in ICd 10?
The ICD-10-CM Official Guidelines for Coding and Reporting state that parentheses “enclose supplementary words that may be present or absent in the statement of a disease or procedure without affecting the code number to which it is assigned.” This is the rule in both the 2019 and the 2020 ICD-10-CM Official Guidelines.
When did the J44.0 change?
To start, let’s take a quick look at the code change effective Oct. 1, 2019. Code J44.0 will add parentheses around the word acute, so the descriptor will look like this: Chronic obstructive pulmonary disease with (acute) lower respiratory infection.
Can you use J44.0 if you have a lower respiratory infection?
In other words, the change clarifies that you may use J44.0 regardless of whether the documentation specifically states the lower respiratory infection is acute.
What is the code for COPD?
If you think about it, J44.0 is a manifestation of the acute lower respiratory tract infection; if bronchitis or pneumonia wasn’t present, the code would be J44.9, COPD, unspecified, instead.
What is a manifestation of COPD?
A manifestation is a condition expressed as a result of something else. Hemiplegia is a manifestation of a stroke, for example; metabolic encephalopathy is a manifestation of severe hyponatremia. Pneumonia is not a manifestation of COPD. It is a manifestation of a lung infection from some pathogenic organism.
Can you be admitted with COPD?
My answer was actually yes to both. First, just having COPD with an acute lower respiratory tract infection is not grounds for admission. In my experience, if a patient with COPD is not experiencing an exacerbation but is thought to require admission for treatment of pneumonia, then the condition that occasioned the admission is clearly ...
Popular Posts:
- 1. icd code for lrft middle finger sagittal band tear
- 2. icd code for anemia
- 3. icd 10 code for uvj stone
- 4. 2016 icd 10 code for mediport insertion
- 5. icd 10 code for status post diverticulitis with recent microperforation
- 6. icd 10 code for osteopenia of forearms
- 7. icd 10 code for peripheral arteriosclerosis
- 8. 2015 icd 9 code for atherosclerosis of the aorta
- 9. icd 9 code for myasthenia gravis
- 10. what is the icd 10 code for seizure activity