ICD-10
The International Classification of Diseases (ICD) is a globally used diagnostic tool for epidemiology, health management and clinical purposes. The ICD is maintained by the World Health Organization (WHO), which is the directing and coordinating authority for health within the United Nations System.
https://en.wikipedia.org › wiki › International_Classification_o...
Diseases of the respiratory system
Respiratory diseases, or lung diseases, are pathological conditions affecting the organs and tissues that make gas exchange difficult in air-breathing animals.
https://en.wikipedia.org › wiki › Respiratory_disease
How to get rid of exercised induced asthma?
- Warm up and cool down before exercising. This will help you lungs get acclimated to the air.
- Avoid working out during cold weather. If you do, cover your mouth and nose.
- Avoid working out when you have a cold or viral infection.
- Always use your inhaler or prescribed medication before you work out.
What is the ICD 10 code for COPD with asthma?
- exposure to environmental tobacco smoke (Z77.22)
- history of tobacco use (Z87.891)
- occupational exposure to environmental tobacco smoke (Z57.31)
- tobacco dependence (F17.-)
- tobacco use (Z72.0)
What are the signs of exercise induced asthma?
- You cough while exercising.
- You develop a noticeable wheeze during or after your workout.
- You become short of breath during or after a workout.
- You experience chest tightness during or after a workout.
- You feel nauseated or have a sore throat during or after a workout.
How to fix exercise induced asthma in kids?
What’s the Rx for exercised-induced asthma?
- Take these before hitting the gym. Short acting beta agonist or bronchodilator: Using this inhaler 10 to 15 minutes before exercise can prevent symptoms.
- An Inhaler for the long haul. Inhaled corticosteroids: Taken daily for long-term treatment of asthma.
- More tricks for preventing the wheeze. ...
Is EIB the same as exercise induced asthma?
Overview. Exercise-induced bronchoconstriction, or EIB, is the preferred term for what was known for years as exercise-induced asthma . Symptoms develop when airways narrow as a result of physical activity. As many as 90 percent of people with asthma also have EIB, but not everyone with EIB has asthma.
How does EIB differ from regular asthma?
EIA describes patients who have underlying asthma, and exercise is a trigger that exacerbates their asthma. EIB describes patients who do not have a history of asthma and who have bronchospasm associated with only exercise. One reason for this differentiation is the treatment of asthma/EIA versus EIB.
Is J45 909 a billable code?
J45. 909 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is exercise induced bronchospasm?
Exercise-induced bronchospasm is an obstruction of transient airflow that usually occurs five to 15 minutes after physical exertion. Although this condition is highly preventable, it is still underrecognized and affects aerobic fitness and quality of life.
Is exercise-induced asthma considered asthma?
Like it sounds, exercise-induced asthma is asthma that is triggered by vigorous or prolonged exercise or physical exertion. Most people with chronic asthma experience symptoms of asthma during exercise. However, there are many people without chronic asthma who develop symptoms only during exercise.
What is the medical term for exercise-induced asthma?
Exercise-induced asthma is a narrowing of the airways in the lungs triggered by strenuous exercise. It causes shortness of breath, wheezing, coughing, and other symptoms during or after exercise. The preferred term for this condition is exercise-induced bronchoconstriction (brong-koh-kun-STRIK-shun).
What is the correct ICD-10 code for asthma?
ICD-10 Code: J45* – Asthma.
What is the ICD-10 diagnosis code for asthma?
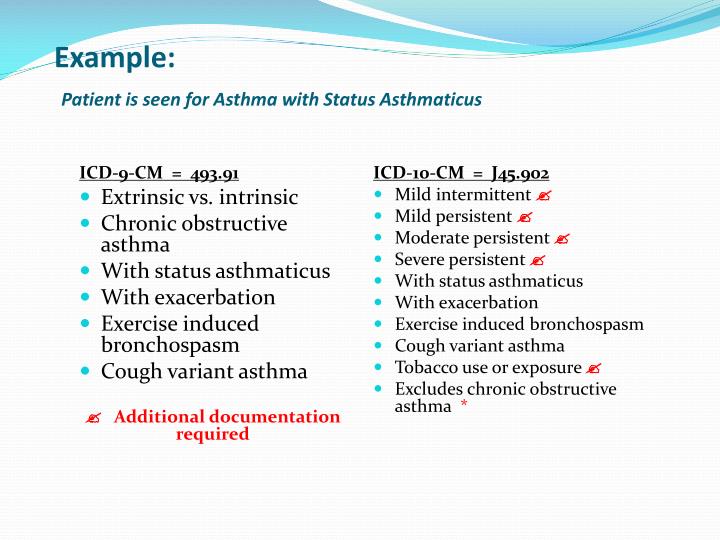
The ICD-CM codes for asthma have changed from 493.00 – 493.99 in ICD-9-CM to J45. 0 – J45. 998 in ICD-10-CM (Table).
What is diagnosis code j449?
9 – Chronic Obstructive Pulmonary Disease, Unspecified.
Is bronchospasm and bronchoconstriction the same?
Bronchospasm is a common diagnosis during anesthesia but it is rarely the correct one. Bronchoconstriction or narrowing of airways from loss of lung volume is a far more common cause of wheezing and difficulty with ventilation during anesthesia.
Is bronchospasm and asthma the same thing?
Bronchospasm vs asthma Bronchospasm is a symptom of asthma and other medical conditions. People with asthma can get bronchospasm, but not everyone with bronchospasm gets asthma. Both conditions are the result of irritated or inflamed airways.
What are the 3 types of asthma?
Types of asthmaDifficult to control asthma.Severe asthma.Occupational asthma.
What is asthma characterized by?
It is characterized by spasmodic contraction of airway smooth muscle, wheezing, and dyspnea (dyspnea, paroxysmal). Asthma is a chronic disease that affects your airways. Your airways are tubes that carry air in and out of your lungs. If you have asthma, the inside walls of your airways become sore and swollen.
When will the ICD-10 J45.909 be released?
The 2022 edition of ICD-10-CM J45.909 became effective on October 1, 2021.
What is the ICd 10 code for asthma?
Refer Chapter 10 (Diseases of the respiratory system (J00- J99) in ICD-10-CM for Asthma guidelines.
Why do you need to code asthma and COPD?
Need to code both asthma and COPD because asthma with additional specificity can be coded along with COPD.
What happens to the lung during asthma?
What happens to our Lungs (Center of respiratory system)during asthma attack: During asthma attack, muscles around the airway gets tighten and the lining inside the airways becomes swollen and produce extra mucus. This makes airway to become narrow and partially block airflow in and out of air sacs.
How many times does asthma occur in a week?
This type of asthma occurs more than 2 times in a week with regular breathing difficulties to an extent of disturbing daily activities. Moderate persistent. These patients suffer from symptoms daily and last for several days. Severe persistent.
Why do asthmatics disappear?
Their symptoms may completely disappear after few years. Experts say this may be due to the growth of airways along with body growth. Cough variant. It is so called because of the main symptom, dry cough. Mild intermittent.
What are the symptoms of asthma?
Asthma causes symptoms like shortness of breath, wheezing, coughing or chest tightness. Severity differs in each person.
What is an inhaler medicine filled?
Inhaler : – Medicine filled inhalers are given to patient to use comfortably at any place when symptoms occurs suddenly.
What is the fifth code for asthma?
A fifth code, J45.9 (Other and unspecified ...) is reserved for forms of the condition that do not fit neatly into the established categories, such as asthmatic bronchitis, childhood asthma, or exercise-induced bronchospasm.
What is the scenario for asthma?
Scenario: Your provider assesses a patient with asthma who is currently experiencing episodes of acute exacerbation. The patient suffers from symptoms at least twice a week, limiting the patient's daily activities somewhat. The patient also uses an inhaler more than twice a week, but not on a daily basis. Based on these symptoms, and the results of a pulmonary function test (PFT) that records a forced expiratory volume in 1 second (FEV1) >80%, your provider diagnoses an acute exacerbation of a mild persistent type of asthma.
What is J45 in pediatrics?
Asthma is probably one of the most common conditions your pediatric practice diagnoses and treats. But no matter how familiar you are with the J45 (Asthma ) code set, it's always a good idea to remind yourself what makes the codes so specific.
What is the J45 code?
Unlike many ICD-10 codes, the J45 code set uses the severity of the symptoms rather than the etiology of the condition as its subdivisions. This is consistent with the current asthma guidelines determined by the NHLBI, which classifies the conditions this way.
What is the highest 5th digit of asthma?
So, you would document the most severe form of an asthma attack, status asthmaticus, with the highest fifth digit, 2. (The J45.90 code set, however, features an exception to that rule, reserving 9 as the sixth digit when the condition is uncomplicated.)
What is the Z77.22 code?
Holle notes that "the use of an additional code such as Z72.0 (Tobacco use), F17- (Nicotine use...), or Z77.22 (Contact with and [suspected] exposure to environmental tobacco smoke [acute] [chronic]) is very important if there is an exposure to smoke or if the patient smokes - and some teens do!"
Popular Posts:
- 1. icd 10 code for strain of lumbar region
- 2. icd 10 code for encounter for pregnancy test
- 3. icd 10 code for left hip x-ray
- 4. icd 10 code for icd 10 code for unspecified fall
- 5. icd 10 code for direct recurrent right inguinal hernia without obstruction
- 6. icd 10 code for other chronic osteomyelitis right ankle and foot
- 7. icd 10 code for oa lumbar
- 8. icd 10 cm code for limb ischemia
- 9. icd 10 code for 611.1
- 10. labs for repeat hcg icd 10 code