Here are the most prevalent codes for speech therapy. Common ICD-10 Codes for Speech Therapy F80.0 — Phonolgoical disorder F80.2 — Mixed receptive-expressive language disorder F80.81 — Childhood onset fluency disorder R13.11 — Dysphagia, oral phase R13.12 — Dysphagia, oropharyngeal phase
Full Answer
What is the diagnosis code for speech therapy?
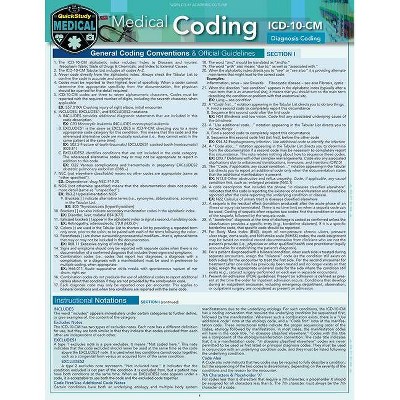
The structure of the codes works like this:
- The first 3 characters in the code identify the category of the disease, disorder, infection, or symptom.
- Characters 4-6 explain where in the body the injury or disease appears, how severe the problem is, and the cause of the injury or disease.
- Character 7 is an extension used for various purposes.
What is the code for speech therapy?
- Documentation of basic hearing evaluation and audiogram;
- Documentation identifying type and extent of hearing loss;
- Documentation of adequate cognitive and memory skills;
- Documentation that visual acuity, with glasses if applicable, is sufficient to allow the beneficiary to participate in the therapy;
What is the ICD9 code for speech therapy?
Speech language pathologists should not report CPT codes 97110, 97112, 97150, 97530, or 97129 as unbundled services included in the services coded as 92507, 92508, or 92526. Please note that cognitive therapy by speech-language pathologists is covered in most Medicare Part B Local Coverage Determinations (LCDs).
What are the evaluation codes for speech therapy?
- Category I describes most of the procedures.
- Category II codes are supplemental tracking codes. These codes are used mainly for performance management.
- Category III codes are temporary codes. They describe emerging and experimental technologies, services, and procedures.

What is the code for speech therapy?
If not, no worries!...Commonly Used CPT Codes for Speech-Language Therapy.Speech, Language, Voice, and Cognition92507Treatment of speech, language, voice, communication, and/or auditory processing disorder; individual92520Laryngeal function studies92521Evaluation of speech fluency (e.g., stuttering, cluttering)14 more rows
Does Medicare pay for 97032?
CPT 97032 (electrical stimulation-manual-each 15 minutes) Medicare does not accept claims for 97032 and 92526 on the same day by speech-language pathologists (see CPT 92526 + CPT 97032 below).
Does Medicare pay for 97129?
In 2020, Medicare removed a single time based cognitive CPT code and replaced it with two codes, the first, 97129 for the initial 15 minutes followed by 97130 for any additional 15 minutes provided.
What is the CPT code for speech screening?
Currently, CPT code 92506 is billed for the evaluation of speech, language, voice, communication, and/or auditory processing.
What is the difference between 97014 and 97032?
97014 — electrical stimulation unattended. (NOTE: 97014 is not recognized by Medicare. Use G0283 when reporting unattended electrical stimulation for other than wound care purposes as described in G0281 and G0282.) 97032 — Application of a modality to one or more areas; electrical stimulation (manual), each 15 minutes.
What is difference between 97014 and G0283?
G0238 is a HCPCS code listing electrical stimulation service and 97014 is a procedure code that is for electrical stimulation. So both of these codes are state the same text but are from different National Coding structures.
How do I bill a Medicare speech pathologist?
SLPs may use 97000 series CPT codes—if appropriate. Under Medicare, SLPs may use CPT codes 97129 (cognitive function intervention, initial 15 minutes) and 97130 (cognitive function intervention, each additional 15 minutes) when treating cognitive disorders.
Can an SLP bill Medicare directly?
Enrollment will allow SLPs in private practice to bill Medicare and receive direct payment for their services. Previously, the Medicare program could only pay SLP services if an institution, physician or nonphysician practitioner billed them.
How do I bill CPT 97129?
Time-Based Codes 97129 represents the first 15 minutes of treatment and can only be billed once per day. Bill 97130 in conjunction with 97129 for each additional 15 minutes of therapy. As an add-on code, 97130 must always be billed in conjunction with 97129 for each additional 15 minutes of therapy, when appropriate.
What is ICD 10 code for speech therapy?
2. F80. 2 — Mixed receptive-expressive language disorder.
What is the ICD 10 code for articulation disorder?
ICD-10-CM Code for Phonological disorder F80. 0.
What is the modifier for speech therapy?
Although there are a number of NCCI-associated modifiers, modifier -59 (distinct procedural service) is the only one used with speech-language pathology related edits. Some payers may require a more specific set of subcategory modifiers. Use these modifiers instead of (not in addition to) modifier -59.
What is the 10th revision of the ICD-10?
The International Classification of Diseases, 10th Revision (ICD-10) is the official system to assign health care codes describing diagnoses and procedures in the United States (U.S). The ICD is also used to code and classify mortality data from death certificates.
When was ICD-10-CM implemented?
ICD-10 was implemented on October 1, 2015, replacing the 9th revision of ICD (ICD-9).
What is the difference between ICD-10 and CM?
The ICD-10-CM has two types of excludes notes. Each note has a different definition for use but they are both similar in that they indicate that codes excluded from each other are independent of each other.
Do SLPs have to report ICD-10 codes?
SLPs practic ing in a health care setting, especially a hospital, may have to code disease s and diagnoses according to the ICD-10. Payers, including Medicare, Medicaid, and commercial insurers, also require SLPs to report ICD-10 codes on health care claims for payment.
New and Revised ICD-10-CM Codes for 2022
Learn about the new and revised codes for fiscal year (FY) 2022, effective October 1, 2021.
ICD-10-CM Code Lists
Audiology and SLP related disorders have been culled from approximately 68,000 codes into manageable, discipline-specific lists. Updated lists are posted annually on October 1.
ICD-10-CM Coding Guidance
Please note that these documents were developed for the October 2015 transition and are no longer being updated. Please refer to current resources for new and revised codes.
What is the code for apaxia of speech?
Apraxia of speech, identified by code R48.2, is a neurological condition where the patient finds it difficult or impossible to move their mouth and tongue to speak. It should not be confused with aphasia, where the person’s inability to speak is due to a problem with understanding or using the words.
What is the code for mixed receptive-expressive language disorder?
Mixed Receptive-Expressive Language Disorder, described by code F80.2, is displayed when a patient has difficulty in expressing their feelings and thoughts and understanding what others are saying. Young children are typically most affected, though it can impact adults as a result of a stroke, seizures, or a traumatic brain injury. Symptoms may vary between patients and include:
What is the term for a person who has trouble swallowing?
Oropharyngeal dysphagia is when a patient has trouble swallowing and the issue involves the patient’s mouth and pharynx (the part of the throat behind the mouth). Symptoms are generally similar to those for the oral phase of dysphagia and include:
What is the code for CAPD?
Code R48.8 is used to capture language deficits as the first-listed diagnosis. It should only be used if an Audiologist has assigned the H93.25 code (Central auditory processing disorder (CAPD)) to a patient. If a diagnosis of CAPD has not been established by an Audiologist, use code F80.2 (mixed receptive-expressive language disorder, developmental) for an auditory processing deficit.
What is the code for swallowing?
Code R13.11 describes difficulty swallowing. Dysphagia is when a patient’s food or liquids take more time and effort to move from their mouth to their stomach. Swallowing may be associated with pain or may not be possible. Dysphagia is more common in older adults. Symptoms include:
What is the ICd 10?
ICD-10 (International Classification of Diseases, Tenth Revision) is a set of codes published by the World Health Organization (WHO) that are used to represent medical diagnoses. An ICD-10 code is assigned to every disease, infection, injury, disorder, and symptom. These codes are used for a variety of purposes, ...
What is the R63.3 code?
Code R63.3 is used for a diagnosis of feeding difficulties and may be used for difficulty clearing the mouth of residue, difficulty establishing feeding, dependency for feeding, chewing finding, and difficulty chewing. This code can be used for developmental delays and sensory food aversions. It excludes feeding problems for newborns and eating disorders.
What happens if you don't meet the medical necessity for speech therapy?
Medical necessity has not been met for billing speech therapy: If medical necessity is not met, the insurance company will deny the claim. All services rendered must be met by medical necessity and have the appropriate ICD-10-CM diagnosis code. If the diagnosis code cannot show the likelihood of the condition or injury, the insurance company will not consider the service appropriate.
What is documentation in speech?
Documentation must include: The ability to execute motor movements needed for speech. Written comprehension and verbal expression. A determination of the patient’s ability to create and communicate expressive thought. An evaluation of the patient’s ability to produce speech sounds.
What is a speech evaluation?
An evaluation of the patient’s ability to produce speech sounds. The physician takes a patient history, including speech and language development, hearing loss, and physical and mental development, and performs a physical examination. Speech and language evaluations are conducted.
What is CPT code 92521?
Finally, let’s go over CPT code 92521. This is one of the most important medical codes for speech therapists. It refers to the evaluation of speech fluency , specifically speech fluency disorders such as stuttering, cluttering, etc.
Popular Posts:
- 1. icd 9 code for scalp woound
- 2. icd 10 code for coccyx fissure
- 3. icd 10 code for early repolarization
- 4. icd 10 code for viral conjunctivitis right eye
- 5. icd 9 code for patellar osteoarthritis
- 6. icd-10 code for no physical injury
- 7. icd 10 code for insect bite left temple
- 8. icd 10 code for mrsa abscess on fecaloma
- 9. icd 10 code for hx lung cancer
- 10. icd 9 code for uterine adhesions