ICD-10 CM code Z79. 83 should be reported for DXA testing while taking medicines for osteoporosis/osteopenia. ICD-10 CM code Z09 should be reported for an individual who has COMPLETED drug therapy for osteoporosis and is being monitored for response to therapy. 4.
What diagnosis covers a DEXA scan?
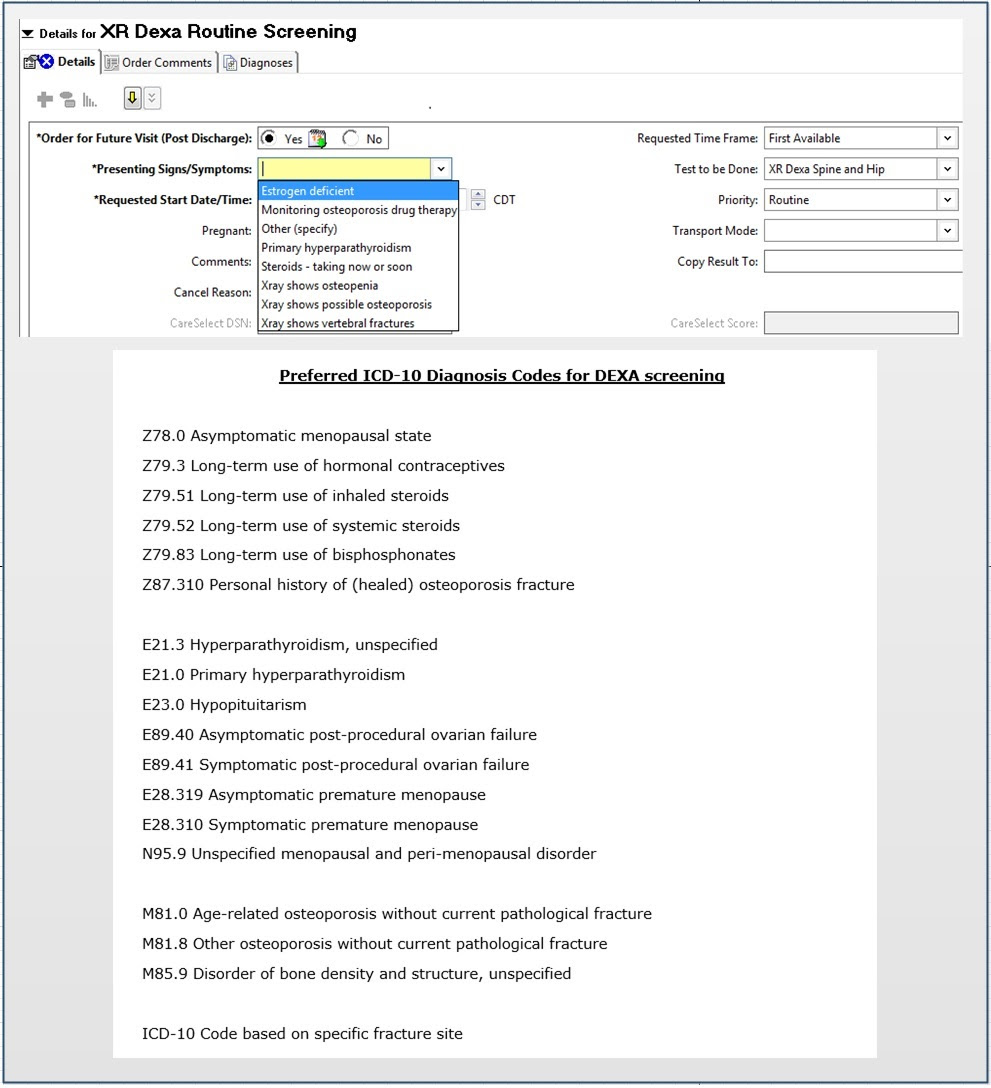
Medicare covers DXA Bone Densitometry for certain Medicare beneficiaries who fall into at least one of the following categories: 1.) A woman whose doctor has determined she's estrogen-deficient and at a clinical risk for osteoporosis, based on her medical history and other findings.
How do you code a DEXA scan?
77085: Dual-energy X-ray absorptiometry (DEXA), bone density study, one or more sites; axial skeleton (e.g., hips, pelvis, spine), including vertebral fracture assessment.
What is the ICD 10 code for bone density scan?
820.
What ICD 10 code covers bone density for Medicare?
(L34639) Bone Mass Measurement ICD-10 Codes That Support Medical Necessity and Covered by Medicare Program: Group 1 Paragraph: Note: ICD-10 codes must be coded to the highest level of specificity.
What is the ICD 10 code for screening for osteoporosis?
Z13. 820 Encounter for screening for osteoporosis - ICD-10-CM Diagnosis Codes.
What is the procedure code for a bone scan?
CPT® 78306, Under Diagnostic Nuclear Medicine Procedures on the Musculoskeletal System.
Is a DEXA scan covered by Medicare?
In most cases, Medicare insurance does cover DEXA scans under Part B. Medicare Part B (Medical Insurance) provides benefits for outpatient procedures that are deemed medically necessary for ongoing treatment of illness.
Is a DEXA scan a bone scan?
A bone density scan uses low dose X-rays to see how dense (or strong) your bones are. You may also hear it called a DEXA scan. Bone density scans are often used to diagnose or assess your risk of osteoporosis, a health condition that weakens bones and makes them more likely to break.
Will Medicare pay for a yearly DEXA scan?
The full cost of a bone density scan is covered under original Medicare every 24 months. If you need to have a bone density test more often, your doctor will have to provide proof of a reason for more frequent testing.
What is the CPT code for a DEXA bone density scan?
Group 1CodeDescription77080DUAL-ENERGY X-RAY ABSORPTIOMETRY (DXA), BONE DENSITY STUDY, 1 OR MORE SITES; AXIAL SKELETON (EG, HIPS, PELVIS, SPINE)77085DUAL-ENERGY X-RAY ABSORPTIOMETRY (DXA), BONE DENSITY STUDY, 1 OR MORE SITES; AXIAL SKELETON (EG, HIPS, PELVIS, SPINE), INCLUDING VERTEBRAL FRACTURE ASSESSMENT1 more row
Is a bone density test considered diagnostic?
A bone density scan is used to: Diagnose osteopenia (low bone mass) Diagnose osteoporosis. Predict risk of future fractures.
Can Z13 820 be a primary diagnosis?
Medicare will always deny Z13. 820 if it is the primary or only diagnosis code.
What does Z12 31 mean?
For example, Z12. 31 (Encounter for screening mammogram for malignant neoplasm of breast) is the correct code to use when you are ordering a routine mammogram for a patient. However, coders are coming across many routine mammogram orders that use Z12. 39 (Encounter for other screening for malignant neoplasm of breast).
What is the Z13.820 code?
Z13.820 is a billable diagnosis code used to specify a medical diagnosis of encounter for screening for osteoporosis. The code Z13.820 is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions. The code is exempt from present on admission (POA) reporting for inpatient admissions to general acute care hospitals.#N#The code Z13.820 describes a circumstance which influences the patient's health status but not a current illness or injury. The code is unacceptable as a principal diagnosis.
What is Medicare code editor?
The Medicare Code Editor (MCE) detects and reports errors in the coding of claims data. The following ICD-10 Code Edits are applicable to this code:
What is a screening test?
Also called: Screening tests. Screenings are tests that look for diseases before you have symptoms. Screening tests can find diseases early, when they're easier to treat. You can get some screenings in your doctor's office. Others need special equipment, so you may need to go to a different office or clinic.
How to check for osteoporosis?
Osteoporosis is a silent disease. You might not know you have it until you break a bone. A bone mineral density test is the best way to check your bone health. To keep bones strong, eat a diet rich in calcium and vitamin D, exercise, and do not smoke.
Is Z13.820 a POA?
Z13.820 is exempt from POA reporting - The Present on Admission (POA) indicator is used for diagnosis codes included in claims involving inpatient admissions to general acute care hospitals. POA indicators must be reported to CMS on each claim to facilitate the grouping of diagnoses codes into the proper Diagnostic Related Groups (DRG). CMS publishes a listing of specific diagnosis codes that are exempt from the POA reporting requirement. Review other POA exempt codes here.
How often does Medicare cover dexa?
Medicare will cover DEXA bone mass measurement once every 2 years on a person who falls into 1 out of the 5 Following categories: 1. A woman who has been determined by her physician to be estrogen-deficient and at clinical risk for osteoporosis. 2.
What is DXA used for?
DXA can also be used to measure peripheral sites, such as the wrist and finger. DXA generates 2 x-ray beams of different energy levels to scan the region of interest and measure the difference in attenuation as the low- and high-energy beams pass through the bone and soft tissue.
How to measure BMD?
DXA is probably the most commonly used technique to measure BMD because of its ease of use, low radiation exposure, and its ability to measure BMD at both the hip and spine. DXA can also be used to measure peripheral sites, such as the wrist and finger. DXA generates 2 x-ray beams of different energy levels to scan the region of interest and measure the difference in attenuation as the low- and high-energy beams pass through the bone and soft tissue. The low energy beam is preferentially attenuated by bone, while the high energy beam is attenuated by both bone and soft tissue. This differential attenuation between the 2 beams allows for correction for the irregular masses of soft tissue, which surround the spine and hip, and therefore the measurement of bone density at those sites.
What is a FRAX assessment?
a. A FRAX Assessment is done to identify patients for BMD testing when any of the following criteria are met:
What is the ICd 9 code for osteopenia?
ICD-9-CM code 733.90 should be reported to indicate osteopenia, (only when billing 77080-DXA), when used to follow treatment with FDA approved osteoporosis medications.
Is CPT 77085 billed for screening?
CPT 77085 should NOT be billed for screening and is not part of the Preventive Benefit. Member cost share will apply when medically necessary criteria are met.
What is a dexa scan?
A dexa scan for a cancer patient is usually performed for staging purposes and is coded using the cancer diagnosis.
Can you add 733.90 to a primary diagnosis?
You may add 733.90 as a secondary diagnosis, but you cannot make it your primary diagnosis. "A screening code may be a first listed code if the reason for the visit is specifically the screening exam. It may also be used as an additional code if the screening is done during an office visit for other health problems.
Can you code a Dexa scan for osteopenia?
Click to expand... Yes. You can code it with osteopenia.
Is screening a DX code?
Sorry there is no confusion here, when the test is ordered as a screening then screening is the first listed dx code regardless of the findings. This per the coding guidelines which are HIPAA mandated to be followed. In addition you are changing the parameters of the test, the patient was asymptomatic upon presentation with no reason to believe there would be anything other than a clean result. If the payer does not pay for the screening then the patient should know this prior to the test. Findings during a screening are incidental to the expectation that the patient would be as healthy as they appear. Incidental findings are always secondary dx codes. Please do not assign dx codes just because it is the one that gets paid!
Can osteopenia be coded with osteopenia?
Yes. You can code it with osteopenia.
Can you code a diagnosis as the first listed?
You absolutely may not code the diagnosis as the first listed you must code screening first listed if the reason for the test was screening. The pate was asymptomatic if this was a screening and you cannot change the parameters of the reason for the test and "make the patient symptomatic" the findings were not expected and not wat was being investigated so the findings are incidental. I am sorry that the patient wil have to pay but they should have known that when they agreed to the screening.
Popular Posts:
- 1. icd 10 code for anal stricture
- 2. icd-10 code for vaginal pain
- 3. icd 10 code for esophageal web
- 4. icd 10 code for laryngeal reflux
- 5. what is the icd 10 code for right femur fracture
- 6. icd-10 code for breast mass
- 7. icd 10 code for elevated tumor markers
- 8. icd 10 code for status post peg tube placement
- 9. icd-10-cm code for congenital macroglossia
- 10. icd 9 code for pyelonephritis in pregnancy