Valid for Submission
| ICD-10: | L73.0 |
|---|---|
| Short Description: | Acne keloid |
| Long Description: | Acne keloid |
What is the ICD 10 code for acne keloid?
Oct 01, 2021 · L73.0 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM L73.0 became effective on October 1, 2021. This is the American ICD-10-CM version of L73.0 - other international versions of ICD-10 L73.0 may differ.
What is acne keloidalis nuchae (AKN)?
ICD-10-CM Code L73.0Acne keloid. ICD-10-CM Code. L73.0. BILLABLE. Billable Code. Billable codes are sufficient justification for admission to an acute care hospital when used a principal …
What is the ICD 10 code for eczematous acne?
L73.0 is a billable diagnosis code used to specify a medical diagnosis of acne keloid. The code L73.0 is valid during the fiscal year 2022 from October 01, 2021 through September 30, 2022 …
Is it folliculitis keloidalis or acne cheloidalis nuchae?
Histology of folliculitis keloidalis. Categories: Pathology, Follicular disorder. Subcategories: Neutrophilic scarring alopecia, Cicatricial alopecia. ICD-10: L73.0. ICD-11: EE60.Y.

What causes acne Keloidalis Nuchae?
Acne keloidalis nuchae develops when inflammatory cells go into your hair follicles on your neck, leading to damage of the follicle wall and the sebaceous or oil-secreting gland. This ruptures the follicle and kickstarts the inflammatory process.Jun 1, 2021
What is the ICD-10 code for keloid?
701.4 - Keloid scar | ICD-10-CM.
What is the ICD-10 code for acne scarring?
Scar conditions and fibrosis of skin
L90. 5 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM L90. 5 became effective on October 1, 2021.
L90. 5 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM L90. 5 became effective on October 1, 2021.
What is diagnosis L700?
L700: Acne vulgaris.
What is the ICD-10 code for acne vulgaris?
L70.0
ACNE VULGARIS (COMMON ACNE) AND CYSTIC ACNE ICD-10: L70. 0.
What is the CPT code for excision of keloid scar?
Treatment of a keloid with radiation therapy (up to 3 fractions) is considered medically necessary as adjunct therapy following surgical excision (initiated within 3 days) when the medically necessary criteria for keloid removal are met.
...
...
| CPT | |
|---|---|
| L91.0 | Hypertrophic scar (keloid) |
What are keloid scars?
A keloid is usually larger than the original wound. A scar that stays inside the bounds of the original wound is a hypertrophic scar. A keloid scar is a thick raised scar. It can occur wherever you have a skin injury but usually forms on earlobes, shoulders, cheeks or the chest.
What is atrophic acne scars?
An atrophic scar develops when the skin cannot regenerate tissue correctly. Unlike keloids and hypertrophic scars, atrophic scars are indented in appearance due to healing that occurs below the expected layer of skin.
Is it a keloid or hypertrophic scar?
What's the difference between a hypertrophic scar and a keloid scar?
| Hypertrophic Scars Versus Keloids | |
|---|---|
| Hypertrophic Scars Versus Keloids | |
| Appearance around wound | Stays within wound area |
| Color | Pink to red |
| Where found on body | More common in taut skin areas |
•
Jun 1, 2021
What is L70 9 acne?
ICD-10 code L70. 9 for Acne, unspecified is a medical classification as listed by WHO under the range - Diseases of the skin and subcutaneous tissue .
What is diagnosis code z79899?
ICD-10 code Z79. 899 for Other long term (current) drug therapy is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is L70 0 acne vulgaris?
ICD-10 Code for Acne vulgaris- L70. 0- Codify by AAPC. Diseases of the skin and subcutaneous tissue. Disorders of skin appendages.
The ICD code L730 is used to code Acne keloidalis nuchae
Acne keloidalis nuchae (also known as "Acne keloidalis", "Dermatitis papillaris capillitii", "Folliculitis keloidalis", "Folliculitis keloidis nuchae", and "Nuchal keloid acne":526) is a destructive scarring folliculitis that occurs almost exclusively on the occipital scalp of people of African descent, primarily men.
ICD-10-CM Alphabetical Index References for 'L73.0 - Acne keloid'
The ICD-10-CM Alphabetical Index links the below-listed medical terms to the ICD code L73.0. Click on any term below to browse the alphabetical index.
Equivalent ICD-9 Code GENERAL EQUIVALENCE MAPPINGS (GEM)
This is the official approximate match mapping between ICD9 and ICD10, as provided by the General Equivalency mapping crosswalk. This means that while there is no exact mapping between this ICD10 code L73.0 and a single ICD9 code, 706.1 is an approximate match for comparison and conversion purposes.
What is the code for acne keloid?
L73.0 is a billable diagnosis code used to specify a medical diagnosis of acne keloid. The code L73.0 is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.
What is keloidal scarring?
ACNE KELOID-. a type of acneiform disorder in which secondary pyogenic infection in and around pilosebaceous structures end s in keloidal scarring. it manifests as persistent folliculitis of the back of the neck associated with occlusion of the follicular orifices. it is most often encountered in black or asian men.
What is the GEM crosswalk?
The General Equivalency Mapping (GEM) crosswalk indicates an approximate mapping between the ICD-10 code L73.0 its ICD-9 equivalent. The approximate mapping means there is not an exact match between the ICD-10 code and the ICD-9 code and the mapped code is not a precise representation of the original code.
What is the name of the disease that causes pimples?
Acne. Also called: Pimples, Zits. Acne is a common skin disease that causes pimples. Pimples form when hair follicles under your skin clog up. Most pimples form on the face, neck, back, chest, and shoulders. Anyone can get acne, but it is common in teenagers and young adults. It is not serious, but it can cause scars.
Can acne cause scars?
Most pimples form on the face, neck, back, chest, and shoulders. Anyone can get acne, but it is common in teenagers and young adults. It is not serious, but it can cause scars.
Can acne scars be on the face?
Most pimples form on the face, neck, back, chest, and shoulders. Anyone can get acne, but it is common in teenagers and young adults. It is not serious, but it can cause scars. No one knows exactly what causes acne. Hormone changes, such as those during the teenage years and pregnancy, probably play a role.
Can acne scars be caused by pregnancy?
Anyone can get acne, but it is common in teenagers and young adults. It is not serious, but it can cause scars. No one knows exactly what causes acne. Hormone changes, such as those during the teenage years and pregnancy, probably play a role. There are many myths about what causes acne.
Introduction
Folliculitis keloidalis (also called folliculitis keloidalis nuchae) is best grouped as one of the neutrophilic scarring alopecias.
Histology of folliculitis keloidalis nuchae
Low power view exhibits a dense superficial and deep inflammatory process with dermal scarring and follicular disruption (Figure 1). There may be variable degrees of overlying scale crust with tufted hair follicles evident as multiple hair shafts within widened follicular infundibulae (Figures 1 and 2).
Special stains in folliculitis keloidalis nuchae
PAS staining should always be performed to exclude a fungal infection.
Differential diagnosis of folliculitis keloidalis nuchae
Folliculitis decalvans: While many features are shared, there is typically significantly less fibrosis in this condition. Clinical discrimination is reliable.
Where do keloid-like papules and plaques occur?
Acne keloidalis nuchae (AKN), or folliculitis keloidalis, is a chronic inflammatory disease in which pustules and keloid-like papules and plaques occur at the nape of the neck, occipital scalp, and sometimes extend up to the vertex scalp.
Where does AKN occur?
Acne keloidalis nuchae (AKN), or folliculitis keloidalis, is a chronic inflammatory disease in which pustules and keloid-like papules and plaques occur at the nape of the neck, occipital scalp, and sometimes extend up to the vertex scalp. Despite its name, it is generally accepted that the lesion is not associated with acne, is not a true keloid, and can occur beyond the nuchal area.
Is AKN rare in women?
AKN has been reported in other racial / ethnic groups, including individuals of Hispanic and Korean descent and White people. Women are rarely affected unless they shave their hair at the nape of the neck. AKN is rare in patients before puberty or after age 50. The condition is often painful and disfiguring.
What causes scarring in hair follicles?
The condition is often painful and disfiguring. Inflammation of the hair follicle and fibrosis of the tissue typically result in scarring, including scarring alopecia. The etiology is unclear; many different hypotheses and factors have been proposed.
What is the complication of Tinea capitis?
Tinea capitis (and its complication, a kerion ) – A dermatophyte infection commonly seen in children. Folliculitis – May affect other hair-bearing areas of the body. Dissecting cellulitis of the scalp – Frequently involves the vertex in addition to the occiput.
What is keloidalis nuchae?
Acne keloidalis nuchae (also known as "acne keloidalis", "dermatitis papillaris capillitii", "folliculitis keloidalis", "folliculitis keloidis nuchae", and "nuchal keloid acne") is a destructive scarring folliculitis that occurs almost exclusively on the occipital scalp of people of African descent, primarily men.
How old is Acne keloidalis nuchae?
Acne keloidalis nuchae most commonly presents itself in individuals aged 13 to 25. The disease is closely related to pseudofolliculitis barbae and both occur frequently in black men in the military, where it is so common that the US Army has developed official protocols for management.
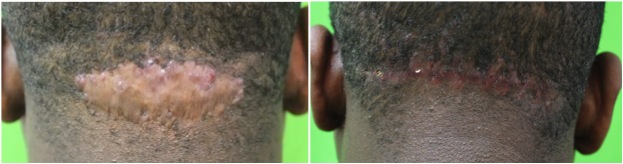
What is the name of the bumps on the back of the neck?
AKN is characterized by firm pink or flesh-colored hyperpigmented bumps in the skin, which are usually located on the back of the back of the neck. This is mainly because men often cut their hair very low as opposed to women, allowing the hair to prick the occipital scalp thereby causing irritation.
Can AKN cause comedones?
Bacterial folliculitis and acne can mimic the appearance of AKN; however, unlike acne, comedones are not seen with AKN. Treatments for AKN aim to reduce inflammation and prevent infections and scarring.
What is the treatment for AKN?
Therapies for AKN may include topical antibiotics, topical or intralesional corticosteroids, and laser hair removal. Recommended modifications to shaving habits include liberal use of shaving cream, avoidance of stretching the skin while shaving, and use of a single-blade razor rather than a razor with multiple blades.
Is Folliculitis keloidalis more common in black people than white people?
Folliculitis keloidalis is more common in dark-skinned people than in whites and most often affects adult Afro-Caribbean males with black curly hair. It is 20 times more common in males than in females.
What is keloidalis in hair?
Some researchers have concluded that folliculitis keloidalis may begin with an injury during a close hair cut or the use of a razor. It is thought to be a mechanical form of folliculitis, in which ingrown hair shafts irritate the wall of the hair follicle resulting in inflammation.
Is folliculitis keloidalis a bacterial infection?
Others argue that folliculitis keloidalis is a primary skin disease unrelated to either ingrown hairs or bacterial infection. An association of folliculitis keloidalis with obesity and metabolic syndrome has been observed in some patients.
Is folliculitis keloidalis a disease?
Others argue that folliculitis keloidalis is a primary skin disease unrelated to either ingrown hairs or bacterial infection. An association of folliculitis keloidalis with obesity and metabolic syndrome has been observed in some patients.
What is the name of the folliculitis that affects the nape of the neck?
Folliculitis keloidalis is an unusual form of chronic folliculitis ( inflammation of hair follicle unit) and cicatricial alopecia (scarring hair loss) that affects the nape of the neck. Folliculitis keloidalis, or folliculitis keloidalis nuchae, is sometimes called acne cheloidalis nuchae or acne keloidalis.
What are the bumps on my hairline?
Sometimes there are pustules around the hair follicles ( folliculitis ). As time goes on the bumps become small scars and then the small scars may greatly enlarge to become keloid-like masses. The scars are hairless and can form a band along the hairline.
Can bumps be keloid?
As time goes on the bumps become small scars and then the small scars may greatly enlarge to become keloid-like masses. The scars are hairless and can form a band along the hairline. Tufted hairs may be present; these are multiple hair shafts emerging from a single follicular opening.
Does Aetna use excimer?
Aetna considers excimer and pulsed dye laser treatment medically necessary for persons with mild-to-moderate localized plaque psoriasis affecting 10 % or less of their body area who have failed to adequately respond to 3 or more months of topical treatments, including at least 3 of the following: Anthralin;
Does Aetna use lasers for psoriasis?
Aetna considers the excimer laser or pulsed dye laser experimental and investigation al in the treatment of forms of psoriasis other than plaque psoriasis because of insufficient evidence in the peer-reviewed literature. Aetna considers laser treatment cosmetic for the following indications (not an all-inclusive list): Pearly penile papules.
Where can plaque psoriasis be found?
Plaque psoriasis can appear on any skin surface, although the knees, elbows, scalp, trunk and nails are the most common locations. There are several other types of psoriasis, and between 10 % and 30 % of people with psoriasis also develop psoriatic arthritis.
Is excimer laser effective for psoriasis?
There is evidence from controlled clinical trials of the effectiveness of excimer laser treatment of mild-to-moderate psoriasis. However, the comparative effectiveness of topical and laser treatment of psoriasis is unknown because these treatments have not been directly compared in a prospective clinical study.
Popular Posts:
- 1. icd 10 cm code for: fall from grocery cart
- 2. icd 10 code for history of a fib
- 3. icd 10 code for cat cry syndrome
- 4. icd-10 code for avr
- 5. icd 10 code for bladder polyp
- 6. icd 10 code for missed medication
- 7. icd 10 code for niemann pick disease
- 8. icd-10 code for history of ruptured cerebral aneurysm
- 9. icd 10 cm code for follow up lower back pain
- 10. icd 10 code for low iodine without goiter