Full Answer
What is the CPT code for anaerobic culture?
Wound Anaerobic Culture Test Includes Isolation and identification (additional CPT coding of 87076, 87077, 87143, or other code depending on methods required) of potential anaerobic and aerobic pathogens; susceptibility testing if culture results warrant at an additional charge.
When is an anaerobic culture indicated in the workup of Enterobacter infections?
Anaerobic culture is especially indicated when an exudate has a foul odor or if the exudate has a grayish discoloration and is hemorrhagic. Frequently, more than one organism is recovered from an anaerobic infection.
What is the CPT code for recovery from anaerobic infections?
Frequently, more than one organism is recovered from an anaerobic infection. The isolation and identification (additional CPT coding of 87076, 87077, 87143 or other code, depending on the methods required) of potential anaerobic and aerobic pathogens Susceptibility testing if culture results warrant at an additional charge.
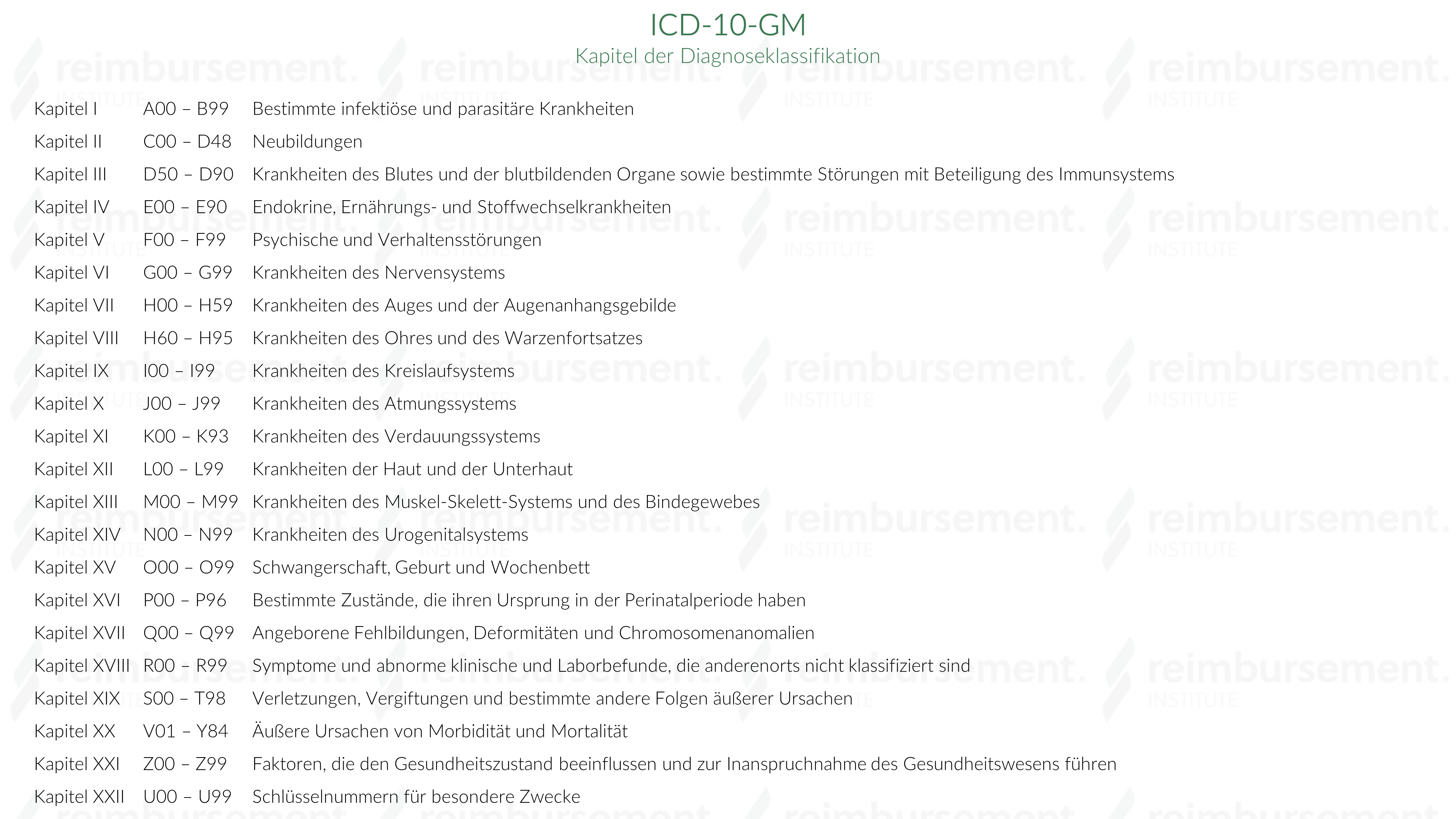
What is the ICD 10 code for other specified bacterial agents?
Other specified bacterial agents as the cause of diseases classified elsewhere 2016 2017 2018 2019 2020 2021 Billable/Specific Code B96.89 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. Short description: Oth bacterial agents as the cause of diseases classd elswhr
What is culture aerobes?
Culture, Aerobic Bacteria - Aerobic bacteria cause a variety of human infections. Proper specimen collection and transport, media and incubation are important criteria for the recovery of aerobes. The primary aerobic bacterial agents of skin and tissue infections include S. aureus, P.
What's an anaerobic culture?
An anaerobic culture means the test is done without letting oxygen get to the sample. Infections caused by anaerobic bacteria can occur almost anywhere in your body. These may be infections in your mouth or lungs, diabetes-related foot infections, infected bites, and gangrene.
What is aerobic culture test?
This test is used to isolate and identify potentially pathogenic aerobic organisms. A susceptibility test will be performed at an additional charge when organisms isolated meet microbiologic criteria for clinical significance.
What is the difference between aerobic and anaerobic specimens?
bacteria are classified as aerobic and anaerobic based on the types of respiration....Aerobic Bacteria vs Anaerobic Bacteria.Difference between Aerobic and AnaerobicAEROBICANAEROBICNeed oxygen to surviveDo not require oxygen to survive4 more rows
How do you send an anaerobic culture?
Swabs or small tissue samples can be inserted into the transport media by removing the cap. The tube is then tightly recapped and sent ASAP to the laboratory. Surgical specimens obtained from usually sterile sites Clean skin first; use syringe to obtain specimen.
What is the difference between aerobic and anaerobic blood culture?
Aerobic – No growth after 48 hours of incubation. Anaerobic – No growth after 72 hours of incubation. Final report – No growth after 7 days. LIMITATIONS A single negative culture does not rule out infection.
How do you get aerobic wound culture?
Swab the wound from margin to margin in a 10-point zigzag fashion. Use enough pressure to express fluid from within the wound tissue. Place the swab in the culture medium, label it according to your facility's policies and procedures, and send it to the lab as soon as possible. Redress the wound as ordered.
How do you determine if a bacteria is aerobic or anaerobic?
Aerobic and anaerobic bacteria can be differentiated by culturing them in test tubes of thioglycollate broth: 1: Obligate aerobes need oxygen because they cannot ferment or respire anaerobically. They gather at the top of the tube where the oxygen concentration is highest.
Is a throat culture aerobic or anaerobic?
Specimens from sites that have anaerobic bacteria as indigenous flora will not be cultured anaerobically (eg, throat, feces, colostomy stoma, rectal swabs, bronchial washes, cervical-vaginal mucosal swabs, sputa, skin and superficial wounds, voided or catheterized urine, ulcer surfaces, drainages onto contaminated ...
What specimen requires anaerobic culture?
Specimens that are suitable for anaerobic culture: Normally sterile body fluids, such as pleural, peritoneal, joint and cerebrospinal fluid, bile, etc. Surgical specimens from sites that normally are sterile. Deep abscess contents taken aseptically. Aspirates from deep wounds.
What is aerobic and Unaerobic bacteria?
Aerobic bacteria refers to the group of microorganisms that grow in the presence of oxygen and thrive in the anoxygenic environment. Anaerobic bacteria refers to the group of microorganisms that grow in the absence of oxygen and cannot survive in the presence of an anoxygenic environment.
Which specimen is suitable for anaerobic cultures?
Materials appropriate for anaerobic culture include blood specimens, aspirates of body fluids (pleural, pericardial, cerebrospinal, peritoneal, and joint fluids), urine collected by suprapubic aspiration, abscess contents, deep wound aspirates, and specimens obtained by special procedures such as transtracheal ...
How long do anaerobes live?
Maintain specimen at room temperature. Specimens for anaerobic culture should be maintained at room temperature. Anaerobes will survive 24 to 72 hours when properly collected in the anaerobic transport tube.
Can you use a red top vacutainer tube?
Sterile tube or other sterile leak-proof container, blood culture bottle, Vacutainer™ Plus no Additive tube; sodium heparin tube, and swabs with visible fluid. Do not use red-top Vacutainer™ tubes.
Clinical Significance
Deep wound/abscess infections are often caused by a mixture of aerobic and anaerobic bacteria.
Test Details
Culture, Aerobic Bacteria and Culture, Anaerobic Bacteria with Gram Stain
What is anaerobic culture?
Anaerobic culture is especially indicated when an exudate has a foul odor or if the exudate has a grayish discoloration and is hemorrhagic. Frequently, more than one organism is recovered from an anaerobic infection.
What sites are inappropriate for anaerobic cultures?
Because of resident anaerobic flora, the following sites are inappropriate for anaerobic cultures and will be rejected: throat and nasopharynx, sputum, bronchoscopy specimens, gastrointestinal contents, voided or catheterized urine, urogenital swabs (eg, vaginal and/or cervical), and specimens from superficial wounds.
What are anaerobic and aerobes?
In open wounds, anaerobic organisms may play an etiologic role, whereas aerobes may represent superficial contamination. Serious anaerobic infections are often due to mixed flora that are pathologic synergists. Anaerobes frequently recovered from closed postoperative wound infections include Bacteroides fragilis, ∼50%; Prevotella melaninogenica, ∼25%; Peptostreptococcus prevotii, ∼15%; and Fusobacterium sp, ∼25%. Anaerobes are seldom recovered in pure culture (10% to 15% of cultures). Aerobes and facultative bacteria when present are frequently found in lesser numbers than the anaerobes. Anaerobic infection is most commonly associated with operations involving opening or manipulating the bowel or a hollow viscus (eg, appendectomy, cholecystectomy, colectomy, gastrectomy, bile duct exploration, etc). The ratio of anaerobes to facultative species is normally about 10:1 in the mouth, vagina, and sebaceous glands and at least 1000:1 in the colon. Biopsy culture is particularly useful in establishing the diagnosis of anaerobic osteomyelitis, 2 clostridial myonecrosis, intracranial actinomycosis, and pleuropulmonary infections. Anaerobic infections of soft tissue include anaerobic cellulitis, necrotizing fasciitis, clostridial myonecrosis (gas gangrene), anaerobic streptococcal myositis or myonecrosis, synergistic nonclostridial anaerobic myonecrosis, and infected vascular gangrene. These infections, particularly clostridial myonecrosis, necrotizing fasciitis, and nonclostridial anaerobic myonecrosis, may be fulminant and are frequently characterized by the presence of gas and foul-smelling necrotic tissue. 3 Empiric therapy based on likely pathogens should be instituted as soon as appropriate cultures are collected.
How long can anaerobic culture be stored?
Under these conditions, aerobes and anaerobes will survive 24 to 72 hours when properly collected in the anaerobic transport tube. Storage of specimens in the ESwab™ transport at room temperature for greater than 48 hours may result in diminished recovery of certain anaerobic species.
How to kill anaerobes?
Some anaerobes will be killed by contact with molecular oxygen for only a few seconds. Overlying and adjacent areas must be carefully disinfected to eliminate contamination with indigenous flora. Ideally, pus or other fluid obtained by needle aspiration through intact skin or mucosal surface that has been cleaned with antiseptic should be collected. Sampling of open lesions is enhanced by deep aspiration using a sterile plastic catheter. Curettings of the base of an open lesion are optimal. If irrigation is necessary, nonbacteriostatic sterile normal saline may be used. Lower respiratory samples must be obtained by transtracheal percutaneous needle aspiration, transbronchial biopsy, transthoracic needle biopsy, or open lung biopsy by physicians trained in these procedures. If swabs must be used, collect two, use one for Gram stain and one for culture. Anaerobic transports must be used for swabs and for aspirates. Specimens are to be collected from a prepared site using sterile technique. Contamination with normal flora from skin, rectum, vaginal tract, or other body surfaces must be avoided.
How to obtain a lower respiratory sample?
Lower respiratory samples must be obtained by transtracheal percutaneous needle aspiration, transbronchial biopsy, transthoracic needle biopsy, or open lung biopsy by physicians trained in these procedures. If swabs must be used, collect two, use one for Gram stain and one for culture. Anaerobic transports must be used for swabs and for aspirates.
What is an unlabeled specimen?
Unlabeled specimen or name discrepancy between specimen and test request label; specimen not received in appropriate anaerobic transport tube; swab not in gel transport medium or ESwab™ transport; swab not stored in oxygen-free atmosphere; specimen refrigerated; specimen received after prolonged delay in transport (usually more than 48 hours). Note: Refrigeration inhibits viability of certain anaerobic organisms. Specimens from sites that have anaerobic bacteria as indigenous flora will not be cultured anaerobically (eg, throat, feces, colostomy stoma, rectal swabs, bronchial washes, cervical-vaginal mucosal swabs, sputa, skin and superficial wounds, voided or catheterized urine, ulcer surfaces, drainages onto contaminated surfaces).
What is anaerobic culture?
Anaerobic cultures are indicated particularly when suspected infections are related to gastrointestinal tract, pelvic organs, associated with malignancy, related to use of aminoglycosides, or occur in a setting in which the diagnosis of gas gangrene or actinomycosis is considered. Anaerobic culture is especially indicated when an exudate has a foul odor or if the exudate has a grayish discoloration and is hemorrhagic. Frequently, more than one organism is recovered from an anaerobic infection.
What is anaerobic infection?
Anaerobic infection is most commonly associated with operations involving opening or manipulating the bowel or a hollow viscus (eg, appendectomy, cholecystectomy, colectomy, gastrectomy, bile duct exploration, etc.).
What is the ratio of anaerobes to facultative species?
The ratio of anaerobes to facultative species is normally about 10:1 in the mouth, vagina, and sebaceous glands and at least 1000:1 in the colon. Biopsy culture is particularly useful in establishing the diagnosis of anaerobic osteomyelitis, 2 clostridial myonecrosis, intracranial actinomycosis, and pleuropulmonary infections.
Can a blood culture be positive?
Blood culture s yield positive results in less than five percent of cases of anaerobic pulmonary infection. Specimens received in anaerobic transport containers are not optimal for aerobic fungus cultures. Mycobacterium sp or Nocardia sp, which may cause abscesses, will not be recovered even if present, since extended incubation periods, ...
Popular Posts:
- 1. icd 9 code for systolic hypertension
- 2. icd-10 code for septic shock unspecified
- 3. what is the icd 10 code for respiratory failure
- 4. icd 9 code for lupus anticoagulant positive
- 5. icd 9 code for allergic reation to eye wash
- 6. icd 10 code for mucinous adenocarcinoma
- 7. icd 10 code for abnormal diagnostic imaging
- 8. icd 10 code for diabetic hyperpigmentation
- 9. icd 10 code for adhd with anxiety
- 10. icd 10 code for breast ca screening