Other intervertebral disc displacement, lumbar region
M51. 26 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM M51. 26 became effective on October 1, 2021.What is the ICD 10 code for disc herniation?
ICD-10-CM Diagnosis Code S06.A1XD Traumatic brain compression with herniation, subsequent encounter Traumatic brain compression with herniation, subs ICD-10-CM Diagnosis Code H11.029 [convert to ICD-9-CM] Central pterygium of unspecified eye Central pterygium ICD-10-CM Diagnosis Code H53.41 Scotoma involving central area Central scotoma
Does a disc herniation heal on its own?
· M51.26 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM M51.26 became effective on October 1, 2021. This is the American ICD-10-CM version of M51.26 - other international versions of ICD-10 M51.26 may differ.
Can I work with herniated disc?
· Thoracic disc herniation; ICD-10-CM M51.24 is grouped within Diagnostic Related Group(s) (MS-DRG v 39.0): 551 Medical back problems with mcc; 552 Medical back problems without mcc; Convert M51.24 to ICD-9-CM. Code History. 2016 (effective 10/1/2015): New code (first year of non-draft ICD-10-CM) 2017 (effective 10/1/2016): No change
Can a Xray diagnose a herniated disc?
ICD-10-CM Diagnosis Code M51.9. Unspecified thoracic, thoracolumbar and lumbosacral intervertebral disc disorder. 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code. ICD-10-CM Diagnosis Code M50.20 [convert to ICD-9-CM] …
.jpg)
What is a central disc herniation?
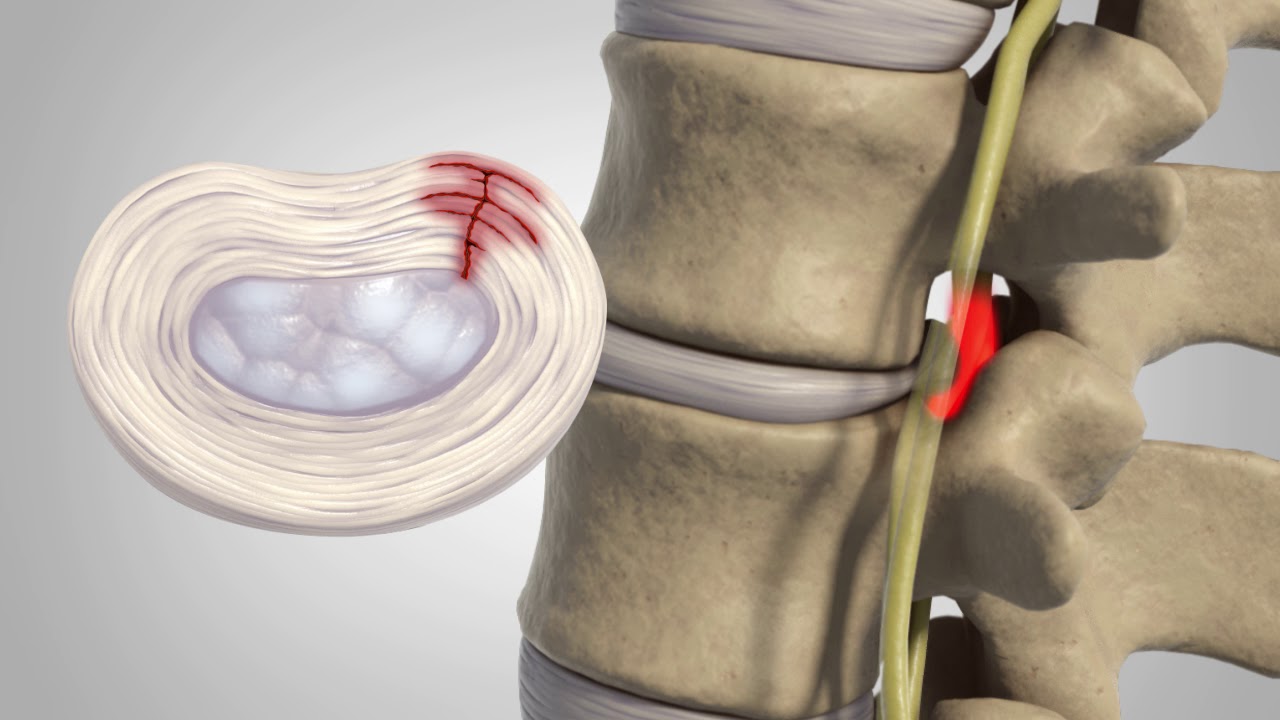
A herniated disc (also called bulged, slipped or ruptured) is a fragment of the disc nucleus that is pushed out of the annulus, into the spinal canal through a tear or rupture in the annulus.
Where is the central disc?
Central: When the disc extrudes into in the spinal cord. Subarticular (Lateral Recess or Paracentral): When the disc extrudes between the spinal cord and the foramen (the space through which the nerves exit the spinal canal). Foraminal (Lateral): Disc extrusion into the foramen.
What is diagnosis code M51 26?
Other intervertebral disc displacement, lumbar regionICD-10 code M51. 26 for Other intervertebral disc displacement, lumbar region is a medical classification as listed by WHO under the range - Dorsopathies .
What is the ICD 10 code for herniated nucleus pulposus?
ICD-10-CM Diagnosis Code K42 K42.
What is central disc protrusion L4-L5?
AN L4-L5 slip disc (herniated or bulged) can impinge (compress) the thecal sac (spinal cord fibers) and spinal nerves. The slightest amount of compression or impingement on a nerve or spinal cord fibers is significant. Nerve compression is significant because it causes nerve degeneration.
What is a focal central disc protrusion?
A bulge involves more than half of the circumference of an intervertebral disc (greater than 180 degrees) whereas a disc herniation involves less than half. A focal disc protrusion occur when its base involves less than 90 degrees of the disc circumference.
Is disc displacement the same as herniated disc?
Disc herniation (termed as intervertebral disc displacement) is a type of spinal disease based on IDD or not, with local pain and/or sciatica due to mechanical compression and autoimmune cascades upon the corresponding nerve roots.
What is medical code M54 16?
16: Radiculopathy Lumbar region.
What is G89 29 diagnosis?
ICD-10 | Other chronic pain (G89. 29)
What is thoracolumbar and lumbosacral intervertebral disc disorder?
Thoracic degenerative disc disease refers to the degeneration, or breakdown, of the shock-absorbing intervertebral discs that cushion the vertebrae in the upper and middle back (called the thoracic spine). It develops most frequently in middle-aged people or young adults with active lifestyles.
What is the nucleus pulposus made of?
Nucleus pulposus is the inner core of the vertebral disc. The core is composed of a jelly-like material that consists of mainly water, as well as a loose network of collagen fibers.
What character is used for disc disorders?
Only use the fourth character “9” for unspecified disc disorders if the documentation does not indicate anything more than the presence of a disc problem. But beware, payors are expected to ask for clarification if unspecified or “NOS” codes are used.
What is the T12-L1 code?
Though it is not specifically mentioned, “thoracolumbar” likely only includes T12-L1, and “lumbosacral” probably only refers to the L5-S1 interspace. There is a strange rule for cervical disc disorders indicating that you should code to the most superior level of the disorder.
What is the 5th character of a disc?
9 = unspecified disc disorder. The fifth character provides detail about the anatomical location within the spinal region. A basic knowledge of spinal anatomy should make fifth-character selection easy, but only if it is documented properly. This includes transitionary regions.
Can a spinal disc be coded?
These spinal disc codes appear to be a bit complex, but with some study and evaluation, the logic used to create them becomes clear. The provider can use the codes to guide proper documentation and the coder then can select the right codes with confidence.
Is sciatica a code for lumbar radiculopathy?
It is already included in the code. Likewise, don’t code sciatica (M54.3-) if you code for lumbar disc with radiculopathy. It would be redundant. On a side note, lumbar radiculopathy (M54.16) might be used if pain is not yet known to be due a disc, but it radiates from the lumbar spine.
What is the objective of decompressing the spinal cord?
Read and be guided by the method being used to decompress the area, remember that various procedures can decompress the spinal cord or spinal nerve roots, but the objective is to release the compression and the root operation assigned is “release.”
What is the procedure to remove a portion of the spinal cord?
There are differing procedures that can accomplish decompression of the spinal cord or spinal nerve roots. These include laminotomy (removal of small portion of lamina)/laminectomy (removal of entire bony lamina); foraminotomy/foraminectomy to remove bone around the neural foramen; discectomy to remove a portion of bulging or herniated or degenerative disc; osteophyte (bony growth or bone spurs) removal; corpectomy to remove all or a part of the body of a vertebra and laminoplasty which is the expansion of the spinal canal by cutting the lamina to release the spinal cord.
When is a decompressive surgery performed?
When a decompressive surgery is performed to relieve pressure on a body part, such as the nerve root or spinal cord, the appropriate root operation will be Release rather than the root operations Excision or Resection.
Is spinal decompression coding complicated?
Spinal procedure coding can be daunting for coders. The spine itself can be quite complicated anatomically and the procedures done to address spinal conditions can be even more complicated! HIA has developed an educational Action Plan to address one of these areas, spinal decompression coding. Below are a few excerpts from that Action Plan.
Popular Posts:
- 1. icd 10 dx code for arthritis in knee
- 2. icd 10 code for bk nephropathy
- 3. icd 10 code for left ring finger deformity
- 4. icd 9 code for tripe palms and florida mucosal acanthosis
- 5. icd 10 code for sciatica left side
- 6. icd-10-pcs code flourescent light treatment for jaundice
- 7. icd-10 code for left knee injury
- 8. icd-10 code for painful urination
- 9. icd 10 code for buckle-handle tear
- 10. what is icd 10 code for afib