1 for chordoma of skull and face, ICD-9 code 170.2 and ICD-10 code C41. 2 for chordoma of vertebral column, ICD-9170.6 ICD-10 C41. 4 for chordoma of sacrum/coccyx.Aug 21, 2020
Full
AnswerWhat is the ICD 10 code for chondromalacia?
C41.0 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2018/19 edition of ICD-10-CM C41.0 became effective on October 1, 2018.
What is Clivus chordoma?
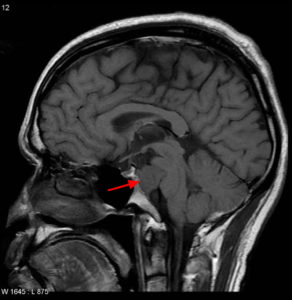
Clivus chordoma Arising from the embryonic rests of the notochord al, clivus chordoma are slow-growing yet aggressively invasive and destructive tumor s.
What is the ICD 10 code for excluded note?
C41.2 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C41.2 became effective on October 1, 2021. This is the American ICD-10-CM version of C41.2 - other international versions of ICD-10 C41.2 may differ. A type 1 excludes note is a pure excludes.
What is the pathophysiology of chordoma of the notochord?
Chordoma is a rare slow-growing neoplasm thought to arise from cellular remnants of the notochord. The evidence for this is the location of the tumors (along the neuraxis ), the similar immunohistochemical staining patterns, and the demonstration that notochordal cells are preferentially left behind in the clivus...
What is Clival chordoma?
Clival chordomas are locally invasive tumors of the midline skull base. Chordoma are locally invasive slow-growing malignant tumors that arise from the remnant of the primitive notochord. They occur most commonly in the skull base (clivus) and lower spine.
What is the ICD-10 code for chondrosarcoma?
Malignant neoplasm of bone and articular cartilage, unspecified. C41. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C41.
What is the ICD-10 code for skull base Mass?
ICD-10-CM Code for Benign neoplasm of bones of skull and face D16. 4.
What is C79 51 ICD-10?
C79. 51 Secondary malignant neoplasm of bone - ICD-10-CM Diagnosis Codes.
What is the ICD 10 code for sarcoma?
Malignant neoplasm of connective and soft tissue, unspecified. C49. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C49.
What is chondrosarcoma?
Chondrosarcoma is a rare type of cancer that usually begins in the bones, but can sometimes occur in the soft tissue near bones. Chondrosarcoma happens most often in the pelvis, hip and shoulder. More rarely, it can happen in the bones of the spine.
What is the clivus bone?
(KLY-vus) A bone at the base of the skull, near the spine. Tumors, such as chordomas and chondrosarcomas, may form on the clivus.
What is a chordoma?
Chordoma is a slow growing cancer of tissue found inside the spine. Chordoma can happen anywhere along the spine. It is most often found near the tailbone (called a sacral tumor) or where the spine meets the skull (called a clival tumor). Chordoma is also called notochordal sarcoma.
What is a clivus lesion?
Clival tumors are growths on the clivus, a portion of bone at the base of the skull. When clival tumors grow, they may invade and damage important nearby structures: cranial nerves, the internal carotid arteries and the brainstem, for example.
What is the ICD-10 code for C79 9?
9: Secondary malignant neoplasm, site unspecified.
What is diagnosis code C90 00?
ICD-10 code: C90. 00 Multiple myeloma Without mention of complete remission.
What is secondary malignant neoplasm of bone?
Secondary bone cancer – This means the cancer started in another part of the body but has now spread (metastasised) to the bone. It may also be called metastatic bone cancer, bone metastases or bone mets.
What does "type 1 excludes" mean?
A type 1 excludes note is for used for when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What chapter is neoplasms classified in?
All neoplasms are classified in this chapter, whether they are functionally active or not. An additional code from Chapter 4 may be used, to identify functional activity associated with any neoplasm. Morphology [Histology] Chapter 2 classifies neoplasms primarily by site (topography), with broad groupings for behavior, malignant, in situ, benign, ...
Notochordal lesions
Cite this page: Hart J. Chordoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechordoma.html. Accessed February 14th, 2022.
Chordoma
Cite this page: Hart J. Chordoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechordoma.html. Accessed February 14th, 2022.
The Clinical Syndrome
Clival chordoma is a rare neoplasm that arises from embryological remnants of the notochord along the spinal axis. Clival chordomas are usually benign, although aggressive clival chordomas have been reported.
Signs and Symptoms
Headache is the most common presenting complaint in patients with clival chordoma. Other common symptoms associated with clival chordoma reflect the propensity of this tumor to compress adjacent neural structures, causing facial pain, facial numbness, facial paresthesias, and diplopia ( Table 21.1 ).
What is expert recommendations for the diagnosis and treatment of chordoma?
Expert Recommendations for the Diagnosis and Treatment of Chordoma is a handbook produced by the Chordoma Foundation, which summarizes recommendations developed by a group of over 40 leading doctors who specialize in caring for chordoma patients. It is available electronically in English, Chinese, Italian, Dutch, and Spanish and hardcopies are available in English and Spanish.
Where is the sacral bone chordoma located?
Sacral Bone Chordoma. Chordomas can arise from bone in the skull base and anywhere along the spine. The two most common locations are cranially at the clivus and in the sacrum at the bottom of the spine.
What happened to Craig Heyward?
While initially thought to be successfully removed, the tumor returned in 2005, and caused Heyward's death in May 2006.
What is the HPS stain for chordoma?
HPS stain. There are three histological variants of chordoma: classic al (or "conventional"), chondroid and dedifferentiated. The histological appearance of classical chordoma is of a lobulated tumor composed of groups of cells separated by fibrous septa. The cells have small round nuclei and abundant vacuolated cytoplasm, ...
What is the antigen for melanoma?
62% of chordomas express the High Molecular Weight Melanoma Associated Antigen, also known as Chondroitin sulfate proteoglycan 4 ( CSPG4) which has been the target of immune therapy. In 2009, scientists discovered that an inherited gene duplication is responsible for the familial form of this disorder.
Which is more effective, x-ray or proton therapy?
The proximity of chordomas to vital neurological structures such as the brain stem and nerves limits the dose of radiation that can safely be delivered. Therefore, highly focused radiation such as proton therapy and carbon ion therapy are more effective than conventional x-ray radiation.
Is chordoma radioresistant?
The decision whether complete or incomplete surgery should be performed primarily depends on the anatomical location of the tumor and its proximity to vital parts of the central nervous system. Chordomas are relatively radioresistant, requiri ng high dos es of radiation to be controlled.
What is a Clivus chordoma?
Clivus chordoma. Arising from the embryonic rests of the notochord al, clivus chordoma are slow-growing yet aggressively invasive and destructive tumor s.
What structures are adjacent to chordomas?
The management of chordomas of the base of the skull is particularly challenging as they lie adjacent to vital anatomic structures, such as the carotid and basilar arteries and the brain stem , which limits surgical access and resectability as well as delivery of high doses of radiation 5) 6).
Can neuraxis spread to distant locations?
They show a strong tendency for local recurrence even after combined surgical and radiosurgical treatment. The possibility of spreading to distant locations of the neuraxis may further complicate the treatment and causes additional morbidity.
Popular Posts:
- 1. icd 10 code for fall hitting head
- 2. icd 10 code for lv apical thrombus
- 3. what is the correct icd 10 code for f10.10
- 4. icd 10 cm code for dyslipidemia,
- 5. icd 10 code for i10
- 6. icd 10 code for atypical skin lesions
- 7. icd 9 code for thyroid screening
- 8. icd 10 code for hypercalcemia due to malignancy
- 9. icd 10 code for trochanter
- 10. icd 10 code for sun sensitivity rash