ICD-10-CM Code for Long term (current) use of opiate analgesic Z79. 891.
What is the life expectancy with chronic opioid use?
We are aware of two prior studies of life expectancy among people who use opioids. One was small, including 106 deaths, finding life expectancy deficits of 9.0 years for men and 17.3 years for women (Hayes et al., 2011). The other included 1005 deaths and focused on people starting methadone treatment in Spain in the 1990s (Brugal et al., 2005).
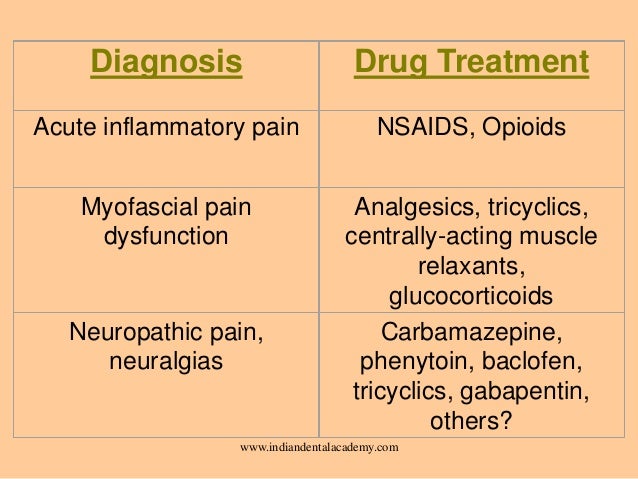
Should opioids be used for chronic non-cancer pain?
Evidence suggests long-term opioid use (greater than three months) for chronic non-cancer pain offers limited benefit. Instead, research suggests pain and physical functioning often improve when opioids are tapered or deprescribed, particularly combined with other treatments such as cognitive and physical therapy.
What is the code for opiate use disorder?
use disorder, only the opioid-induced depressive disorder code is given, with the 4th character indicating whether the comorbid opioid use disorder is mild, moderate, or severe: F11.14 for mild opioid use disorder
Does chronic pain and opioid use determine politics?
The increase in use of strong morphine-type drugs (opioids) for the treatment of chronic pain is an area of much concern, particularly in North America . Termed an "opioid epidemic," most developed countries have seen a major increase in opioid prescribing over the last decade or so.
What is the ICD-10 code for chronic continuous use of opioids?
Long term (current) use of opiate analgesic Z79. 891 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z79. 891 became effective on October 1, 2021.
What is the ICD-10 code for opioid dependence?
Opioid dependence, uncomplicated F11. 20 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM F11. 20 became effective on October 1, 2021.
What is long term current use of opiate analgesic?
Although opioids can be beneficial, they are also commonly associated with adverse events, such as sedation, constipation, and respiratory depression. Their long-term use can lead to physiologic tolerance and addiction.
What is the ICD-10 code for chronic pain?
89.29 or the diagnosis term “chronic pain syndrome” to utilize ICD-10 code G89. 4. If not documented, other symptom diagnosis codes may be utilized. Note: ICD-10 code Z45.
What is diagnosis code Z51 81?
ICD-10 code Z51. 81 for Encounter for therapeutic drug level monitoring is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is the F code for opiates?
Table 4ICD-9-CM and ICD-10-CM diagnosis codes defining opioid use disorder (OUD)Diagnosis codeDescriptionICD-9-CM diagnosis codesOpioid useF11.90Opioid use, unspecified, uncomplicatedF11.920Opioid use, unspecified with intoxication, uncomplicated138 more rows
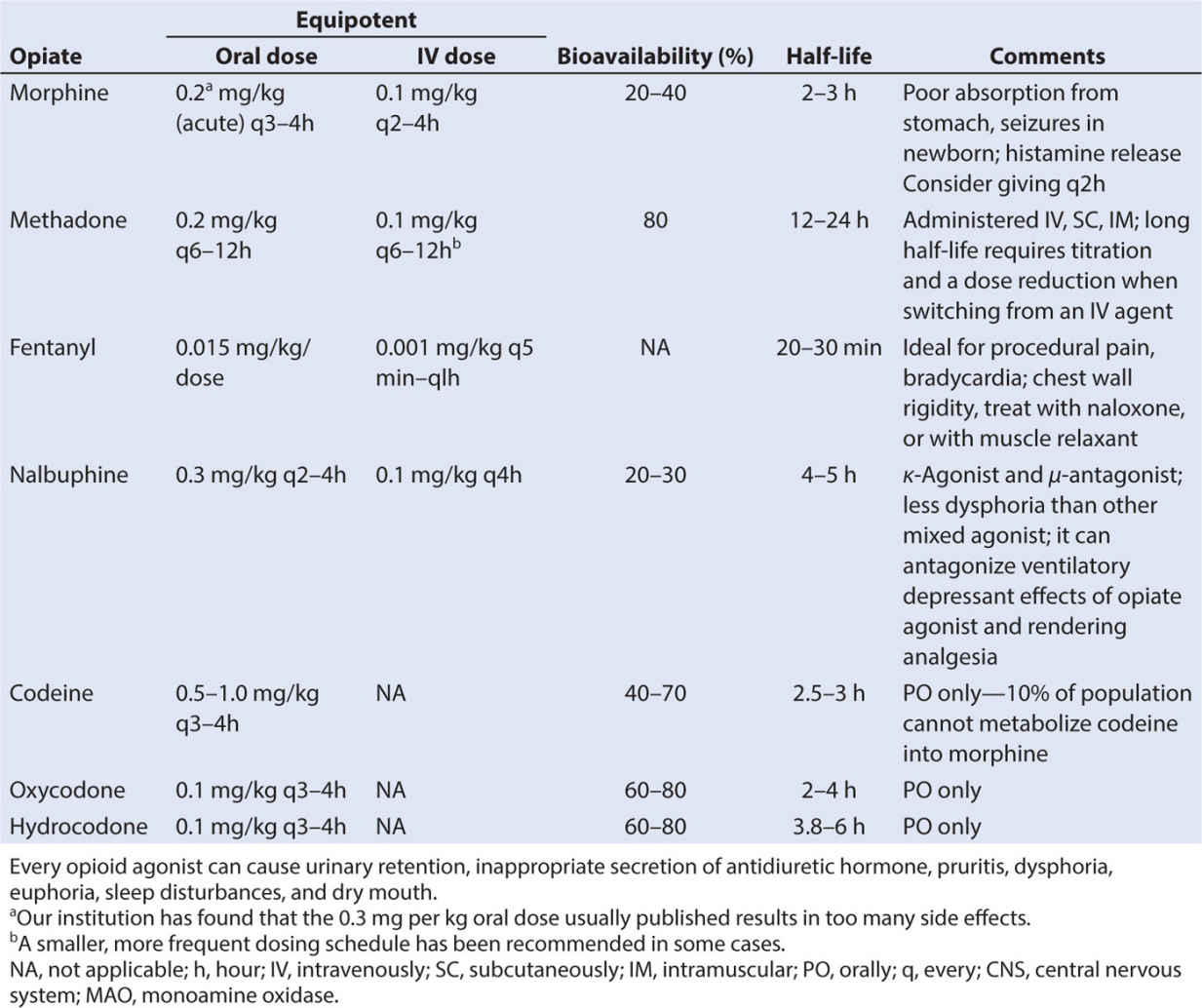
What are examples of opioid analgesics?
These opioids include tramadol, oxycodone, fentanyl, methadone, dextromethorphan, meperidine, codeine, and buprenorphine.
What are the 5 A's of monitoring chronic opioid response?
For this reason, we recommend Five A's of assessment: Analgesia, Activity, Adverse reactions, Aberrant behavior and Affect. Every person for whom opioids are prescribed has the potential to abuse their medication (Webster & Dove, 2007).
What is the DSM 5 code for opioid use disorder?
14 for mild opioid use disorder with opioid-induced depressive disorder or F11. 24 for a moderate or severe opioid use disorder with opioid- induced depressive disorder. Specify current severity: 305.50 (F11.
What is the ICD 10 code for chronic?
Chronic pain, not elsewhere classified The 2022 edition of ICD-10-CM G89. 2 became effective on October 1, 2021. This is the American ICD-10-CM version of G89.
Can chronic pain be a primary diagnosis?
Only report pain diagnosis codes from the G89 category as the primary diagnosis when: The acute or chronic pain and neoplasm pain provide more detail when used with codes from other categories; or. The reason for the service is for pain control or pain management.
How do you code acute on chronic pain?
Category G89 includes codes for acute pain, chronic pain, and neoplasm-related pain, as well as codes for two pain syndromes. In order for you to assign these codes, the physician must document that the pain is acute, chronic, or neoplasm-related.
What is the ICd 10 code for opioid use?
Tolerance for opioids. Withdrawal symptoms when opioids are not taken. In ICD-10-CM, opioid use, abuse, and dependence are coded to category F11.
What is the diagnosis of opioid use disorder?
Per the Diagnostic and Statistical Manual of Mental Disorders (DSM–5): The diagnosis of Opioid Use Disorder can be applied to someone who has a problematic pattern of opioid use leading to clinically significant impairment or distress, ...
What is the meaning of "failing to carry out important roles at home, work or school because of opioid use"
Failing to carry out important roles at home, work or school because of opioid use. Continuing to use opioids, despite use of the drug causing relationship or social problems. Giving up or reducing other activities because of opioid use. Using opioids even when it is physically unsafe.
Why do you need a query when coding opioid use disorders?
Because provider documentation is not always detailed enough to support proper code assignment, a query may be needed when coding opioid use disorders, to attain any missing pertinent information.
How many people die from opioids every day?
Opioid abuse, addiction, and overdoses are a serious public health problem. According to the National Institute on Drug Abuse, more than 115 people in the United States die after overdosing on opioids, every day.
What is the meaning of "taking more opioids than intended"?
Taking more opioid drugs than intended. Wanting or trying to control opioid drug use without success. Spending a lot of time obtaining, taking, or recovering from the effects of opioid drugs. Cravings opioids. Failing to carry out important roles at home, work or school because of opioid use.
How much is the economic burden of opioids?
The Centers for Disease Control and Prevention estimates that the “economic burden” of prescription opioid misuse (including the costs of healthcare, lost productivity, addiction treatment, and criminal justice involvement) in the United States equals $78.5 billion a year. Opioid use, opioid abuse, and opioid dependence are grouped together as ...
What is billable code?
Billable codes are sufficient justification for admission to an acute care hospital when used a principal diagnosis. The Center for Medicare & Medicaid Services (CMS) requires medical coders to indicate whether or not a condition was present at the time of admission, in order to properly assign MS-DRG codes.
Is a diagnosis present at time of inpatient admission?
Diagnosis was present at time of inpatient admission. Yes. N. Diagnosis was not present at time of inpatient admission. No. U. Documentation insufficient to determine if the condition was present at the time of inpatient admission. No.
Popular Posts:
- 1. icd 10 code for hsv type 1
- 2. what is the icd 10 code for hematuria
- 3. icd 10 code for unobstruced nephrolithiasis
- 4. icd 10 code for abnormal ultrasound of pelvis
- 5. icd 10 code for injury of left ankle
- 6. icd 10 code for r35.0
- 7. icd 10 code for status post bowel resection
- 8. icd-10 code for skin tag removal
- 9. icd 9 code for rejection of kidney transplant
- 10. icd 10 code for encounter for therapeutic drug level monitoring