1 Dysthymia. A chronic depression of mood, lasting at least several years, which is not sufficiently severe, or in which individual episodes are not sufficiently prolonged, to justify a diagnosis of severe, moderate, or mild recurrent depressive disorder (F33. -).
Is F34 1 a billable diagnosis?
F34. 1 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the correct ICD-10 code for depression?
ICD-Code F33. 0 is a billable ICD-10 code used for healthcare diagnosis reimbursement of major depressive disorder.
What is the ICD-10-CM code for dysthymia?
ICD-10 Code for Dysthymic disorder- F34. 1- Codify by AAPC.
What is F33 diagnosis?
1 Recurrent depressive disorder, current episode moderate. A disorder characterized by repeated episodes of depression, the current episode being of moderate severity, as in F32. 1, and without any history of mania.
What is depression F32 A?
F32. Major depressive disorder, single episode In typical, mild, moderate, or severe depressive episodes the patient suffers from lowering of mood, reduction of energy and decrease in activities.
What is code for depression?
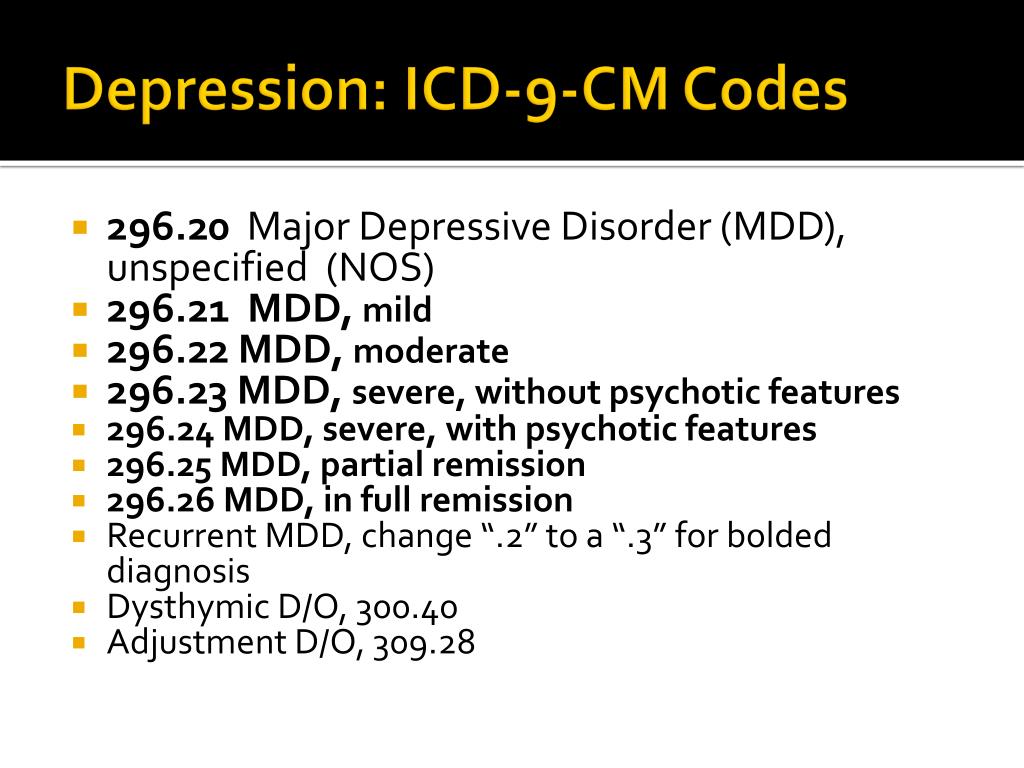
Multiple diagnosis codes exist for coding for depression. The most general is 311, “Depressive disorder, not elsewhere classified.” Code 290.21 represents senile dementia with depressive features.
What is diagnosis code F43 21?
ICD-10 code F43. 21 for Adjustment disorder with depressed mood is a medical classification as listed by WHO under the range - Mental, Behavioral and Neurodevelopmental disorders .
What is meant by dysthymia?
Overview. Persistent depressive disorder, also called dysthymia (dis-THIE-me-uh), is a continuous long-term (chronic) form of depression. You may lose interest in normal daily activities, feel hopeless, lack productivity, and have low self-esteem and an overall feeling of inadequacy.
What does F43 23 mean?
23 – Adjustment Disorder with Mixed Anxiety and Depressed Mood. ICD-Code F43. 23 is a billable ICD-10 code used for healthcare diagnosis reimbursement of Adjustment Disorder with Mixed Anxiety and Depressed Mood. Its corresponding ICD-9 code is 309.28.
What is code f33 2?
2 Recurrent depressive disorder, current episode severe without psychotic symptoms.
What is the ICD-10 code for minor depression?
Code F32. 0 is the diagnosis code used for Major depressive disorder, single episode, mild. This falls under the category of mood [affective] disorders.
Introduction
A meta-analysis of epidemiological studies investigating chronic pain revealed prevalence estimates from 8.7 to 64.4 percent depending on how chronic pain was defined ( Steingrímsdóttir et al., 2017 ). Lifetime prevalence of pain complaints ranges from 24 to 37% ( Bair et al., 2003 ).
Materials and Methods
This is a retrospective study and a re-analysis of the data of Pieh et al. (2012). Data were collected from patients with chronic not malignant pain, treated in the pain clinic in Weiden, Germany, between 2006 and 2010. The study was conducted in accordance with the Declaration of Helsinki and ethical laws were applied.
Results
Of the 496 included patients (254 women) 13 did not complete the treatment due to medical complications. Between 4 (ADS; 0.8% of the total sample) and 9 (PPS-S; 1.8% of the total sample) of the patients did not complete the measures at pre-treatment.
Discussion
In the current study, we investigated the relationship between pre-treatment depression and pain outcomes after a pain treatment in chronic pain patients with regard to the way depression was operationalized (interview-based or questionnaire-based according to the CES-D).
Conclusion
The way depression was operationalized did not influence whether depression predicts pain outcomes or not.
Data Availability
Data regarding this study will not be shared, because clinical data was investigated and we made an agreement with the clinic for not to publish participant data, but only analyses and interpretations.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and ethical laws were applied. All participants signed a consensus declaration and agreed to the analysis of their anonymous data.
Popular Posts:
- 1. icd-9 code for hcg
- 2. icd 10 code for deponia
- 3. icd-10 code for mri brain with and without contrast
- 4. icd 10 code for acute gastroenterieis
- 5. icd 10 code for labaral repair
- 6. icd 10 cm code for for upper lid swelling
- 7. icd 9 code for myelocele
- 8. icd-10-cm code for scabies
- 9. icd 10 code for h pylori infec
- 10. icd 10 code for abscess back left leg