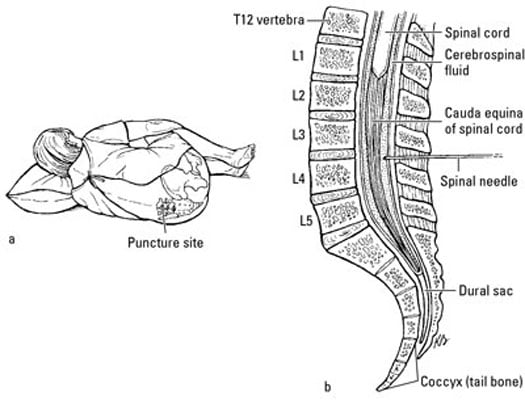
Abnormal cytological findings in cerebrospinal fluid
R83. 6 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM R83. 6 became effective on October 1, 2021.How do you code abnormal findings in cerebrospinal fluid (R83)?
To code a diagnosis of this type, you must use one of the nine child codes of R83 that describes the diagnosis 'abnormal findings in cerebrospinal fluid' in more detail. ICD-10-CM Alphabetical Index References for 'R83 - Abnormal findings in cerebrospinal fluid'
What is the ICD 10 code for abnormal cerebrospinal fluid?
2018/2019 ICD-10-CM Diagnosis Code R83.5. Abnormal microbiological findings in cerebrospinal fluid. R83.5 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD 10 code for Type 1 excludes?
R83.5 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM R83.5 became effective on October 1, 2021. This is the American ICD-10-CM version of R83.5 - other international versions of ICD-10 R83.5 may differ. A type 1 excludes note is a pure excludes.
See more
What is the ICD 10 code for CSF leak?
ICD-10 code G96. 0 for Cerebrospinal fluid leak is a medical classification as listed by WHO under the range - Diseases of the nervous system .
What is the ICD 10 code for fluid collection?
ICD-10 code E87. 70 for Fluid overload, unspecified is a medical classification as listed by WHO under the range - Endocrine, nutritional and metabolic diseases .
What is the ICD 10 code for screening?
9.
What is the diagnosis code for delivery?
9 Multiple delivery, unspecified.
What is the ICD-10 code for R18 8?
ICD-10 code R18. 8 for Other ascites is a medical classification as listed by WHO under the range - Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
What is the ICD-10 PCS code for IV hydration?
The objective of this article is to examine the coding of hydration with CPT® codes 96360, Intravenous infusion, hydration; initial, 31 minutes to 1 hour, and 96361, Intravenous infusion, hydration; each additional hour. The purpose of hydration intravenous (IV) infusion is to hydrate.
What is diagnosis code Z71 89?
Other specified counselingICD-10 code Z71. 89 for Other specified counseling is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What does code Z12 31 mean?
For example, Z12. 31 (Encounter for screening mammogram for malignant neoplasm of breast) is the correct code to use when you are ordering a routine mammogram for a patient. However, coders are coming across many routine mammogram orders that use Z12.
What does code Z12 11 mean?
Z12. 11: Encounter for screening for malignant neoplasm of the colon.
What is code Z3A 39?
ICD-10 code Z3A. 39 for 39 weeks gestation of pregnancy is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
How do you code complications?
For a condition to be considered a complication, the following must be true: It must be more than an expected outcome or occurrence and show evidence that the provider evaluated, monitored, and treated the condition. There must be a documented cause-and-effect relationship between the care given and the complication.
When do you use O80?
Normal Delivery, ICD-10-CM Code O80 Full-term uncomplicated delivery ICD-10-CM code O80 should be assigned when a patient is admitted for a full-term normal delivery and delivers a single, healthy infant without any complications antepartum, during the delivery or postpartum.
What is the ICD 10 code for pelvic fluid collection?
ICD-10-CM Code for Intra-abdominal and pelvic swelling, mass and lump R19. 0.
What is the ICD 10 code for pleural effusion?
ICD-10 Code for Pleural effusion in other conditions classified elsewhere- J91. 8- Codify by AAPC.
What is the ICD 10 code for paracentesis?
R18.8The main diagnosis ICD 10 code for Abdominal paracentesis is R18. 8 (ICD 9 code 789.59) for ascites. This is main reason for performing paracentesis. Medical Coders should report the CPT code 49084, to denote peritoneal lavage, including imaging guidance, when performed.
What is the ICD 10 code for abdominal ascites?
R18. 8 - Other ascites | ICD-10-CM.
What is the ICd 10 code for cerebrospinal fluid?
R83.9 is a billable diagnosis code used to specify a medical diagnosis of unspecified abnormal finding in cerebrospinal fluid. The code R83.9 is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.#N#The ICD-10-CM code R83.9 might also be used to specify conditions or terms like cerebrospinal fluid examination abnormal or csf chemistry abnormal.#N#Unspecified diagnosis codes like R83.9 are acceptable when clinical information is unknown or not available about a particular condition. Although a more specific code is preferable, unspecified codes should be used when such codes most accurately reflect what is known about a patient's condition. Specific diagnosis codes should not be used if not supported by the patient's medical record.
When to use R83.9?
Unspecified diagnosis codes like R83.9 are acceptable when clinical information is unknown or not available about a particular condition. Although a more specific code is preferable, unspecified codes should be used when such codes most accurately reflect what is known about a patient's condition.
Popular Posts:
- 1. icd-10 code for bilateral hearing loss
- 2. patient is seen for the first time for an abrasion of the scalp. icd-10-cm code(s): _____.
- 3. icd 10 code for adhd inattentive
- 4. icd code for patient with history of alcoholism currently in remission
- 5. i dont know what to put for an icd 9 code
- 6. what is the icd 10 code for strep pharyngitis
- 7. icd 10 cm code for hx splenic artery aneurysm
- 8. icd 10 code for hsil pap
- 9. icd 9 code for mrsa in wound
- 10. icd-10 code for guillotine