Common colorectal screening diagnosis codes
| ICD-10-CM | Description |
| Z12.11 | Encounter for screening for malignant ne ... |
| Z80.0 | Family history of malignant neoplasm of ... |
| Z86.010 | Personal history of colonic polyps |
G0105, Colorectal cancer screening; colonoscopy on individual at high risk. Z12. 11, Encounter for screening for malignant neoplasm of colon.Apr 20, 2022
Full
AnswerWhat does ICD 10 do you use for EKG screening?
The specific amount you’ll owe may depend on several things, like:
- Other insurance you may have
- How much your doctor charges
- Whether your doctor accepts assignment
- The type of facility
- Where you get your test, item, or service
What are the criteria for high risk colonoscopy?
“High risk” includes factors such a personal history of colon cancer, inflammatory bowel disease, or adenomatous polyps, or a family history of familial adenomatous polyposis or nonpolyposis colorectal cancer. What is the anesthesia code for colonoscopy?
What is the ICD 10 diagnosis code for CHF?
ICD-10-CM assumes a causal relationship and this is coded as hypertensive heart disease with CHF and an additional code for the specific type of heart failure. In this case, the PDX of hypertensive heart disease with CHF (I11.0) is reported as the PDX followed by the code for the heart failure (I50.9) Under the Category I50 in the ICD-10-CM ...
What is the ICD 10 diagnosis code for?
The ICD-10-CM is a catalog of diagnosis codes used by medical professionals for medical coding and reporting in health care settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates.
How do you code high risk colon cancer screening?
For Medicare beneficiaries, use Healthcare Common Procedural Coding System (HCPCS) code G0105 (Colorectal cancer screening; colonoscopy on individual at high risk) or G0121 (Colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk) as appropriate.
What is the ICD code for screening colonoscopy?
A screening colonoscopy should be reported with the following International Classification of Diseases, 10th edition (ICD-10) codes: Z12. 11: Encounter for screening for malignant neoplasm of the colon.
What does Medicare consider high risk for colonoscopy?
Medicare covers a screening colonoscopy once every 24 months for people considered high risk,9 defined as having a history or a close relative with a history of colorectal polyps or cancer, a history of polyps, or inflammatory bowel disease like Crohn's disease or ulcerative colitis.
What is a Z12 11?
Z12. 11 encounter for screening for malignant neoplasm of colon.
How do you code a surveillance colonoscopy?
There are 2 different sets of screening colonoscopy codes:G0121- Colorectal cancer screening (non-high-risk)G0105-Colorectal cancer screening (high-risk)
What is the difference between screening and surveillance colonoscopy?
Medicare and most insurance carriers will pay for screening colonoscopies once every 10 years. Surveillance colonoscopies are performed on patients who have a prior personal history of colon polyps or colon cancer. Medicare will pay for these exams once every 24 months.
How often will Medicare pay for a high risk colonoscopy?
Colonoscopies. Medicare covers screening colonoscopies once every 24 months if you're at high risk for colorectal cancer. If you aren't at high risk, Medicare covers the test once every 120 months, or 48 months after a previous flexible sigmoidoscopy. There's no minimum age requirement.
How do I bill for a patient seen in our office prior to a screening colonoscopy with no GI symptoms and who is otherwise healthy?
How do I bill for a patient seen in our office prior to a screening colonoscopy with no GI symptoms and who is otherwise healthy? A visit prior to a screening colonoscopy for a healthy patient is not billable.
Does Medicare require prior authorization for colonoscopy?
Many people have extra coverage. However, Medicare requires prior authorization for a colonoscopy before most advantage plans start paying. Pre-approval means your doctor must get a green light before sending you to a Gastroenterologist.
What does Z12 12 mean?
ICD-10 code Z12. 12 for Encounter for screening for malignant neoplasm of rectum is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What does code Z12 31 mean?
For example, Z12. 31 (Encounter for screening mammogram for malignant neoplasm of breast) is the correct code to use when you are ordering a routine mammogram for a patient.
When should Z12 11 be used?
If the patient presents for a screening colonoscopy and a polyp or any other lesion/diagnosis is found, the primary diagnosis is still going to be Z12. 11, Encounter for screening for malignant neoplasm of colon. The coder should also report the polyp or findings as additional diagnosis codes.
What is screening for asymptomatic disease?
Screening is the testing for disease or disease precursors in asymptomatic individuals so that early detection and treatment can be provided for those who test positive for the disease. Type 1 Excludes. encounter for diagnostic examination-code to sign or symptom. Use Additional.
When will the ICD-10 Z12.11 be released?
The 2022 edition of ICD-10-CM Z12.11 became effective on October 1, 2021.
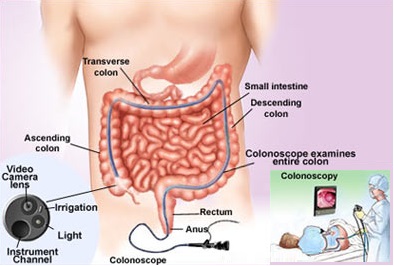
What is colonoscopy procedure?
Definition of Terms Colonoscopy: A colonoscopy is a procedure that permits the direct examination of the mucosa of the entire colon by using a flexible lighted tube. The procedure is done with sedation in a hospital outpatient department, in a clinic , or an office facility. During the colonoscopy a doctor can biopsy and remove pre – cancerous ...
What can a doctor do during a colonoscopy?
During the colonoscopy a doctor can biopsy and remove pre – cancerous polyps and some early stage cancers and also diagnose other conditions or diseases. General definitions of procedure indications from various specialty societies , including the ACA: * A screening colonoscopy is done to look for disease, such as cancer, ...
What is the introduction section of a medical policy?
Note:The Introduction section is for your general knowledge and is not to be takenas policy coverage criteria. The rest of the policy uses specific words and concepts familiar to medical professionals. It is intended for providers.A provider can be a person, such as a doctor, nurse, psychologist, or dentist.
Can a colonoscopy be done during a biopsy?
It can also be doneas a diagnostic procedure when symptoms or lab tests suggest there might be a problem in the rectum or colon.In some cases, minor procedures may be done during a colonoscopy,such as taking a biopsy or destroying an area of unhealthy tissue (a lesion).
Is colonoscopy a screening test?
This guideline applies only to people of average risk. Colonoscopy is only one of the screening tests that can be used. This benefit coverage guideline provides general information about how the health plan decides whether a colonoscopy is covered under the preventive or diagnostic (medical) benefits.
How often does Medicare cover colonoscopy?
Screening colonoscopy: once every 24 months (unless a screening flexible sigmoidoscopy has been performed and then Medicare may cover a screening colonoscopy only after at least 47 months) Screening barium enema (when used instead of a flexible sigmoidoscopy or colonoscopy): once every 24 months.
How often does Medicare cover a flexible sigmoidoscopy?
Screening flexible sigmoidoscopy: once every 48 months (unless the beneficiary does not meet the criteria for high risk of developing colorectal cancer and the beneficiary has had a screening colonoscopy within the preceding 10 years, in which case Medicare may cover a screening flexible sigmoidoscopy only after at least 119 months have passed following the month that the beneficiary received the screening colonoscopy)
What is modifier 33 for sedation?
Append modifier 33 or PT to moderate sedation codes G0500 and +99153 when moderate sedation is furnished in conjunction with screening colonoscopy services to waive the patient’s Medicare copayment/coinsurance and deductible.
What is the second leading cause of cancer-related deaths in the United States?
What better time to refresh your coding know-how for colorectal cancer screening than National Colorectal Cancer Awareness month? Of cancers that affect both men and women, colorectal cancer is the second leading cause of cancer-related deaths in the United States, according to the Centers for Medicare & Medicaid Services (CMS).
Is 00812 deductible or coinsurance?
The deductible and coinsurance will be waived for new CPT code 00812 Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum; screening colonoscopy beginning Jan. 1, 2018, and for claims with new CPT code 00811 Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum; not otherwise specified the deductible will be waived when submitted with modifier PT.
Who is Renee Dustman?
Renee Dustman, BS, AAPC MACRA Proficient, is managing editor - content & editorial at AAPC. She holds a Bachelor of Science degree in Media Communications - Journalism. Renee has more than 30 years' experience in journalistic reporting, print production, graphic design, and content management. Follow her on Twitter @dustman_aapc.
Does Medicare cover barium enemas?
For screening colonoscopies, fecal occult blood tests (FOBTs), flexible sigmoidoscopies, and barium enemas, coverage applies to all Medicare patients who fall into at least one of the following categories:
How often is a colonoscopy performed?
At a frequency of once every 10 years (i.e., at least 119 months have passed following the month in which the last covered HCPCS G0121 screening colonoscopy was performed.)
What is the CPT code for colonoscopy?
Effective January 1, 2018, anesthesia services furnished in conjunction with and in support of a screening colonoscopy are reported with CPT code 00812 and coinsurance and deductible are waived. When a screening colonoscopy becomes a diagnostic colonoscopy, anesthesia services are reported with CPT code 00811 and with the PT modifier; only the deductible is waived.
What is the sensitivity of a blood based screening test?
proven test performance characteristics for a blood-based screening test with both sensitivity greater than or equal to 74% and specificity greater than or equal to 90% in the detection of colorectal cancer compared to the recognized standard (accepted as colonoscopy at this time), as minimal threshold levels, based on the pivotal studies included in the FDA.
How often should you have a flexible sigmoidoscopy?
Once every 48 months (i.e., at least 47 months have passed following the month in which the last covered screening flexible sigmoidoscopy was performed)
How often is a biomarker test required for Medicare?
Effective for dates of service on or after January 19, 2021, a blood-based biomarker test is covered as an appropriate colorectal cancer screening test once every 3 years for Medicare beneficiaries when performed in a Clinical Laboratory Improvement Act (CLIA)-certified laboratory, when ordered by a treating physician and when all of the following requirements are met:
What is an ABN in Medicare?
An ABN may be used for services which are likely to be non-covered, whether for medical necessity or for other reasons. Refer to CMS Publication 100-04, Medicare Claims Processing Manual, Chapter 30, for complete instructions.
When did CPT 00810 become effective?
Effective January 1, 2015 through December 31, 2017, anesthesia professionals who furnish a separately payable anesthesia service (CPT code 00810) in conjunction with a screening colonoscopy shall include the following on the claim for the services that qualify for the waiver of coinsurance and deductible:
What is the A53573 code?
On 8/27/14 Palmetto issued a Local Coverage Article (A53573) that was effective on 8/4/14 with the coverage limited to the ICD codes previously listed. During today's Palmetto webcast, I submitted a question whether they are going to pay claims prior to 8/4/14 and was told that they have no plans to reprocess those claims. They directed me the CPIL, which contains no updates. They have also not issued updates concerning the Local Coverage Article in the Medicare Advisory Bulletin. They stated they are still "awaiting further clarification from CMS."
How long do you have to edit a wiki?
This is a community-maintained wiki post containing the most important information from this thread. You may edit the Wiki once you have been on AAPC for 30 days and have made 5 posts. Learn More
What is the ICD-9 code for Palmetto?
G0105 and G0120 when billed with previously covered ICD-9 codes. Palmetto
What states are J11?
Thanks for the info. This seems to be only affecting Jurisdiction 11 (J11)- Palmetto GBA- North Carolina, South Carolina, Virginia, West Virginia.
What is a family history code?
Family history codes are for use when a patient has a family member (s)who has had a particular disease that causes the patient to be at higher risk of also contracting the disease.
What are the two types of V codes?
There are two types of history ?V? codes, personal and family. Personal history codes explain a patient?s past medical condition that no longer exists and is not receiving any treatment, but that has the potential for recurrence, and therefore may require continued monitoring. Family history codes are for use when a patient has a family member (s) who has had a particular disease that causes the patient to be at higher risk of also contracting the disease. The exceptions to this general rule are category V14, personal history of allergy to medicinal agents and subcategory v15.0, Allergy, other than to medicinal agents. (etc?)
Does Palmetto GBA notify CMS?
Palmetto GBA will notify CMS about this issue.

Popular Posts:
- 1. icd 10 code for complication of cesarean section wound
- 2. icd 10 code for left side hemiparesis due to cva
- 3. icd 10 code for recent history of electric shock
- 4. 2019 icd 10 code for sphenoid sinus opacification
- 5. icd 10 code for decubitus ulcer scral stage 1
- 6. icd-10-cm code for periumbilical abdominal pain
- 7. icd 10 code for traumatic iritis left eye
- 8. icd 10 procedure code for repair of fracture of femur with intramedullary rodding
- 9. icd 10 code for hyperglycemia unspecified
- 10. icd 10 code for history of alzheimer's dementia