ICD-10-CM Code for Personal history of irradiation Z92. 3.
What is the ICD 10 code for history of irradiation?
Personal history of irradiation. Z92.3 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD 10 code for present on admission?
This "Present On Admission" (POA) indicator is recorded on CMS form 4010A. Z92.3 is a billable ICD code used to specify a diagnosis of personal history of irradiation. A 'billable code' is detailed enough to be used to specify a medical diagnosis.
What is the ICD 10 code for potential health hazards?
Z77-Z99 Persons with potential health hazards related to family and personal history and certain conditions influencing health status Z92.3 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2021 edition of ICD-10-CM Z92.3 became effective on October 1, 2020.
What is the Z code for diagnosis?
A corresponding procedure code must accompany a Z code if a procedure is performed. Categories Z00-Z99 are provided for occasions when circumstances other than a disease, injury or external cause classifiable to categories A00 -Y89 are recorded as 'diagnoses' or 'problems'. This can arise in two main ways:
What is the ICD 10 code for radiation?
ICD-10 code Z51. 0 for Encounter for antineoplastic radiation therapy is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is the ICD 10 code for History of brachytherapy?
89.
What is the ICD 10 code for late effect of radiation?
909.2 - Late effect of radiation. ICD-10-CM.
What is DX R68 89?
ICD-10 code R68. 89 for Other general symptoms and signs is a medical classification as listed by WHO under the range - Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
What is ICD-10 code for History of chemotherapy and radiation?
ICD-10 code Z92. 21 for Personal history of antineoplastic chemotherapy is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
How many times can you bill 77263?
77263 is only billable once per course of treatment.
What is the sequencing order when coding a sequela late effect?
Coding of sequela generally requires two codes sequenced in the following order: The condition or nature of the sequela is sequenced first. The sequela code is sequenced second.
What is XRT medical?
XRT: Medical abbreviation for radiotherapy.
What is antineoplastic radiation therapy?
1) Antineoplastic drugs are one of three potential modalities in the treatment of cancer. The other two are surgery and radiation therapy. Antineoplastics can be used as primary treatment in tumors not amenable to surgery or radiation such as leukemia or in widespread metastatic disease.
Is R68 89 billable code?
R68. 89 is a VALID/BILLABLE ICD10 code, i.e it is valid for submission for HIPAA-covered transactions. R68. 89 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is Z00 01?
ICD-10 code Z00. 01 for Encounter for general adult medical examination with abnormal findings is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What does anemia D64 9 mean?
Code D64. 9 is the diagnosis code used for Anemia, Unspecified, it falls under the category of diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism.
What is the Z92.3 code?
Z92.3 is a billable diagnosis code used to specify a medical diagnosis of personal history of irradiation. The code Z92.3 is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.
How many cancer patients receive radiation?
About half of all cancer patients receive it. The radiation may be external, from special machines, or internal, from radioactive substances that a doctor places inside your body. The type of radiation therapy you receive depends on many factors, including. The type of cancer.
Can radiation therapy cause cancer?
Other factors, such as your age and other medical conditions. Radiation therapy can damage normal cells as well as cancer cells. Treatment must be carefully planned to minimize side effects. Common side effects include skin changes and fatigue. Other side effects depend on the part of your body being treated.
Is Z92.3 a POA?
Z92.3 is exempt from POA reporting - The Present on Admission (POA) indicator is used for diagnosis codes included in claims involving inpatient admissions to general acute care hospitals. POA indicators must be reported to CMS on each claim to facilitate the grouping of diagnoses codes into the proper Diagnostic Related Groups (DRG). CMS publishes a listing of specific diagnosis codes that are exempt from the POA reporting requirement. Review other POA exempt codes here.
What is the ICd 10 code for irradiation?
Z92.3 is a valid billable ICD-10 diagnosis code for Personal history of irradiation . It is found in the 2021 version of the ICD-10 Clinical Modification (CM) and can be used in all HIPAA-covered transactions from Oct 01, 2020 - Sep 30, 2021 .
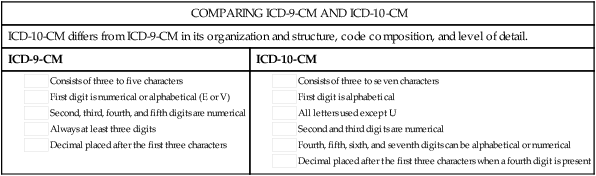
Do you include decimal points in ICD-10?
Some clearinghouses may remove it for you but to avoid having a rejected claim due to an invalid ICD-10 code, do not include the decimal point when submitting claims electronically. See also: History.
What is billable code?
Billable codes are sufficient justification for admission to an acute care hospital when used a principal diagnosis. The Center for Medicare & Medicaid Services (CMS) requires medical coders to indicate whether or not a condition was present at the time of admission, in order to properly assign MS-DRG codes.
What does "type 1 excludes" mean?
Type-1 Excludes mean the conditions excluded are mutually exclusive and should never be coded together. Excludes 1 means "do not code here.". Exposure to radiation in the physical environment - instead, use code Z77.12. Occupational exposure to radiation - instead, use code Z57.1.
What is inclusion term?
Inclusion Terms are a list of concepts for which a specific code is used. The list of Inclusion Terms is useful for determining the correct code in some cases, but the list is not necessarily exhaustive.
Is a diagnosis present at time of inpatient admission?
Diagnosis was present at time of inpatient admission. Yes. N. Diagnosis was not present at time of inpatient admission. No. U. Documentation insufficient to determine if the condition was present at the time of inpatient admission. No.
What is the ICd 10 code for cancer?
For more context, consider the meanings of “current” and “history of” (ICD-10-CM Official Guidelines for Coding and Reporting; Mayo Clinic; Medline Plus, National Cancer Institute):#N#Current: Cancer is coded as current if the record clearly states active treatment is for the purpose of curing or palliating cancer, or states cancer is present but unresponsive to treatment; the current treatment plan is observation or watchful waiting; or the patient refused treatment.#N#In Remission: The National Cancer Institute defines in remission as: “A decrease in or disappearance of signs or symptoms of cancer. Partial remission, some but not all signs and symptoms of cancer have disappeared. Complete remission, all signs and symptoms of cancer have disappeared, although cancer still may be in the body.”#N#Some providers say that aromatase inhibitors and tamoxifen therapy are applied during complete remission of invasive breast cancer to prevent the invasive cancer from recurring or distant metastasis. The cancer still may be in the body.#N#In remission generally is coded as current, as long as there is no contradictory information elsewhere in the record.#N#History of Cancer: The record describes cancer as historical or “history of” and/or the record states the current status of cancer is “cancer free,” “no evidence of disease,” “NED,” or any other language that indicates cancer is not current.#N#According to the National Cancer Institute, for breast cancer, the five-year survival rate for non-metastatic cancer is 80 percent. The thought is, if after five years the cancer isn’t back, the patient is “cancer free” (although cancer can reoccur after five years, it’s less likely). As coders, it’s important to follow the documentation as stated in the record. Don’t go by assumptions or averages.
What is tamoxifen used for?
Tamoxifen and aromatase inhibitor therapy are used on invasive breast cancer to prevent recurrence of the original, invasive cancer.
What is the ICd 10 code for primary malignancy?
According to the ICD-10 guidelines, (Section I.C.2.m):#N#When a primary malignancy has been excised but further treatment, such as additional surgery for the malignancy, radiation therapy, or chemotherapy is directed to that site, the primary malignancy code should be used until treatment is complete.#N#When a primary malignancy has been excised or eradicated from its site, there is no further treatment (of the malignancy) directed to that site, and there is no evidence of any existing primary malignancy, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy.#N#Section I.C.21.8 explains that when using a history code, such as Z85, we also must use Z08 Encounter for follow-up examination after completed treatment for a malignant neoplasm. This follow-up code implies the condition is no longer being actively treated and no longer exists. The guidelines state:#N#Follow-up codes may be used in conjunction with history codes to provide the full picture of the healed condition and its treatment.#N#A follow-up code may be used to explain multiple visits. Should a condition be found to have recurred on the follow-up visit, then the diagnosis code for the condition should be assigned in place of the follow-up code.#N#For example, a patient had colon cancer and is status post-surgery/chemo/radiation. The patient chart notes, “no evidence of disease” (NED). This is reported with follow-up code Z08, first, and history code Z85.038 Personal history of other malignant neoplasm of large intestine, second. The cancer has been removed and the patient’s treatment is finished.
What is adjuvant therapy?
Adjuvant therapy may be chemotherapy, radiation, or hormonal therapy. Adjuvant treatment is given after primary treatment has been completed to either destroy remaining cancer cells that may be undetectable; or to lower the risk that the cancer will come back. The purpose of adjuvant medicine may be:
What is a neoadjuvant?
For example: Neoadjuvant chemotherapy is medicine administered before surgery to reduce the size of a tumor, and possibly provide more treatment options. Adjuvant means “in addition to” and refers to medicine administered after surgery for treatment of cancer. Adjuvant therapy may be chemotherapy, radiation, or hormonal therapy. ...
What is preventative cancer?
Preventative or Prophylactic – to keep cancer from reoccurring in a person who has already been treated for cancer or to keep cancer from occurring in a person who has never had cancer but is at increased risk for developing it due to family history or other factors.
What is a follow up code?
This follow-up code implies the condition is no longer being actively treated and no longer exists. The guidelines state: Follow-up codes may be used in conjunction with history codes to provide the full picture of the healed condition and its treatment. A follow-up code may be used to explain multiple visits.
Popular Posts:
- 1. icd 10 cm code for secondary infection of lower lip).
- 2. icd 10 code for fsecond visit to primary dysmenorrhea
- 3. icd 10 code for h53.9
- 4. icd 10 code for hx colon ca
- 5. icd 10 code for bilateral inguinal lymphadenopathy
- 6. icd 10 cm code for step on object
- 7. 2017 icd 10 code for amputation right fingers
- 8. icd 10 code for mass submandibular
- 9. what is the icd 10 code for chronic ulcer on the right heel skin only
- 10. icd 10 cm code for asdh