E22. 2 - Syndrome of inappropriate secretion of antidiuretic hormone. ICD-10-CM.
What is the ICD 10 code for hyponatremia?
Hyponatremia; Hyponatremia (low sodium level); Hyposmolality; syndrome of inappropriate secretion of antidiuretic hormone (E22.2); Sodium [Na] deficiency ICD-10-CM Diagnosis Code P74.22 [convert to ICD-9-CM]
What are the signs and symptoms of hyponatremia?
A mild but rapid fall in sodium levels can cause severe symptoms like delirium, confusion, and seizures, while chronic but significant hyponatremia (less than 125 mEq/L) may produce mild or no symptoms.
What does SIADH stand for in medical terms?
A 'billable code' is detailed enough to be used to specify a medical diagnosis. Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is characterized by excessive release of antidiuretic hormone from the posterior pituitary gland or another source.
How common is hyponatremia in alcoholics?
Hyponatremia is a common electrolyte abnormality in hospitalized patients with a history of chronic alcoholism. As the study conducted by Liamis, et al. showed 17.3% of hospitalized chronic alcoholics have severe hyponatremia [2].
What is hyponatremia secondary to SIADH?
As its name implies, patients with SIADH have unregulated secretion of vasopressin despite hypotonicity of the serum. Consequently, water intake combined with a high concentration of vasopressin leads to antidiuresis eventually resulting in hyponatremia.
Is hyponatremia and SIADH the same?
SIADH consists of hyponatremia, inappropriately elevated urine osmolality (>100 mOsm/kg), and decreased serum osmolality in a euvolemic patient.
Is SIADH primary or secondary?
The term “primary SIADH” is used for all above-mentioned causes involving a known or suspected dysregulation of OSM and/or circulating-blood volume. The term “secondary SIADH” is attributed to pituitary-independent causes of AVP increases, e.g. in hormone-active neoplasms such as small-cell lung cancer.
What is the ICD-10 code for SIADH?
ICD-10 code E22. 2 for Syndrome of inappropriate secretion of antidiuretic hormone is a medical classification as listed by WHO under the range - Endocrine, nutritional and metabolic diseases .
What is SIADH diagnosis?
SIADH can occur secondary to medications, malignancy, pulmonary disease, or any disorder involving the central nervous system. Diagnosis is made on the basis of clinical euvolaemic state with low serum sodium and osmolality, raised urine sodium and osmolality, and exclusion of pseudohyponatraemia and diuretic use.
What is the sodium level in SIADH?
Both the disorders share few features like inappropriately high urine osmolality in the presence of hyponatremia, high urine sodium (often more than 40 meq/L) and reduced serum uric acid concentration.
Is SIADH a diagnosis of exclusion?
The causes of inappropriate ADH are attributable either to paraneoplastic secretion or to ADH from the posterior pituitary and hypothalamus in response to other, so-called 'nonosmotic' stimuli [Schrier and Berl, 1975]. SIADH is now no longer a diagnosis merely of exclusion.
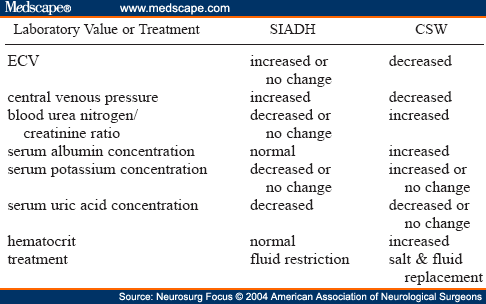
How can you tell the difference between CSW and SIADH?
The key difference is that SIADH is a euvolemic to mildly hypervolumic state, whereas CSW is a volume-depleted state. Unfortunately, the volume status is not always clinically apparent in every patient.
What is the cause of SIADH?
SIADH tends to occur in people with heart failure or people with a diseased hypothalamus (the part of the brain that works directly with the pituitary gland to produce hormones). In other cases, a certain cancer (elsewhere in the body) may produce the antidiuretic hormone, especially certain lung cancers.
Is I10 a billable code?
ICD-Code I10 is a billable ICD-10 code used for healthcare diagnosis reimbursement of Essential (Primary) Hypertension. Its corresponding ICD-9 code is 401.
What is reset Osmostat?
Reset osmostat (RO) consists of a change in the normal plasma osmolality threshold (reduction or increase), which consequently induces chronic dysnatremia (hyponatremia or hypernatremia).
What is the ICD-10 code for adrenal insufficiency?
40.
What is the most common cause of euvolemic hyponatremia in hospitalized patients?
The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is the most common cause of euvolemic hyponatremia in hospitalized patients. A second action of AVP is to cause arteriolar vasoconstriction and a rise in arterial blood pressure, the pressor effect.
What is the syndrome of inappropriate antidiuretic hormone secretion?
Furthermore, what happens in Siadh? Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is a condition in which the body makes too much antidiuretic hormone (ADH). This hormone helps the kidneys control the amount of water your body loses through the urine.
Popular Posts:
- 1. icd 10 code for anxiety with somatization
- 2. icd 10 code for recurrent major depression in remission
- 3. icd 10 cm code for cerebrovascular accident and aspiration
- 4. icd 10 code for hilar lymphadenopathy
- 5. icd-10 code for visual disturbance
- 6. icd 10 code for primary malignant renal pelvis tumor
- 7. 2015 icd 10 code for hydronephrosis with hydroureter
- 8. icd 10 diagnosis code for bulging lumbar disc
- 9. icd 10 code for z47.89
- 10. icd 10 code for adult