C79. 4 Secondary malignant neoplasm of other and unspecified parts of nervous system.
Secondary malignant neoplasm
Secondary malignant neoplasm is a malignant tumor whose cause is the treatment (usually radiation or chemotherapy) which was used for a prior tumor. It must be distinguished from Metastasis from the prior tumor or a relapse from it since a secondary malignant neoplasm is a different tumor.
https://en.wikipedia.org › Secondary_malignant_neoplasm
How do you code leptomeningeal carcinomatosis?
Oct 01, 2021 · C79.49 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C79.49 became effective on October 1, 2021. This is the American ICD-10-CM version of C79.49 - other international versions of ICD-10 C79.49 may differ. All neoplasms are classified in this chapter ...
What is leptomeningeal carcinoma?
Oct 01, 2021 · The 2022 edition of ICD-10-CM C79.31 became effective on October 1, 2021. This is the American ICD-10-CM version of C79.31 - other international versions of ICD-10 C79.31 may differ. All neoplasms are classified in this chapter, whether they are functionally active or not.
What is the CPT code for malignant neoplasm?
Oct 01, 2021 · C79.51 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C79.51 became effective on October 1, 2021. This is the American ICD-10-CM version of C79.51 - other international versions of ICD-10 C79.51 may differ. All neoplasms are classified in this chapter ...
What is the ICD 10 code for secondary malignant neoplasm?
Oct 01, 2021 · C79.32 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C79.32 became effective on October 1, 2021. This is the American ICD-10-CM version of C79.32 - other international versions of ICD-10 C79.32 may differ. All neoplasms are classified in this chapter ...
What is the ICD-10 code for brain metastasis?
C79. 31 - Secondary malignant neoplasm of brain | ICD-10-CM.
What is the ICD-10 code for metastatic cancer?
The 2022 edition of ICD-10-CM C79. 9 became effective on October 1, 2021. This is the American ICD-10-CM version of C79.
What is the code for metastasis?
Code C80. 0, Disseminated malignant neoplasm, unspecified, is for use only in those cases where the patient has advanced metastatic disease and no known primary or secondary sites are specified.Dec 3, 2018
What is the ICD-10 code for primitive neuroectodermal tumor?
The 2022 edition of ICD-10-CM C72. 9 became effective on October 1, 2021.
Is metastatic cancer primary or secondary?
Metastatic cancer has the same name as the primary cancer. For example, breast cancer that spreads to the lung is called metastatic breast cancer, not lung cancer. It is treated as stage IV breast cancer, not as lung cancer.Nov 10, 2020
What is the CPT code for metastatic cancer?
If the site of the primary cancer is not documented, the coder will assign a code for the metastasis first, followed by C80. 1 malignant (primary) neoplasm, unspecified. For example, if the patient was being treated for metastatic bone cancer, but the primary malignancy site is not documented, assign C79. 51, C80.Oct 5, 2017
What is diagnosis code Z51 11?
2022 ICD-10-CM Diagnosis Code Z51. 11: Encounter for antineoplastic chemotherapy.
What is C79 51 ICD-10?
51: Secondary malignant neoplasm of bone.
What is the ICD-10 code for metastatic small cell carcinoma?
C34. 90 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C34. 90 became effective on October 1, 2021.
What is primitive neuroectodermal tumor?
Primitive neuroectodermal tumors (PNETs) are rare, malignant tumors thought to arise from primitive nerve cells. Several treatment options are available; treatment typically includes a combination of surgery, radiation therapy, chemotherapy, and possibly shunt placement.
What is a Esthesioneuroblastoma?

Listen to pronunciation. (es-THEE-zee-oh-NOOR-oh-blas-TOH-muh) A rare type of cancer that forms in the tissues of the upper part of the nasal cavity (space inside the nose). This area is near the bone that separates the nasal cavity from the brain.
What is paraspinal neuroblastoma?
Neuroblastoma may be found in the adrenal glands and paraspinal nerve tissue from the neck to the pelvis. Neuroblastoma most often begins in infancy. It is usually diagnosed between the first month of life and age five years. It is found when the tumor begins to grow and cause signs or symptoms .Jun 10, 2021
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
When will the ICd 10 C79.31 be released?
The 2022 edition of ICD-10-CM C79.31 became effective on October 1, 2021.
What is a C7B tumor?
secondary carcinoid tumors ( C7B.-) secondary neuroendocrine tumors ( C7B.-) A malignant neoplasm that has spread to the brain from another anatomic site or system. The majority are carcinomas (usually lung or breast carcinomas). Cancer that has spread from the original (primary) tumor to the brain.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
Is colorectal cancer metastatic?
Colorectal cancer, metastatic to brain. Colorectal malignant neoplasm metastatic to brain. Secondary malignant neoplasm of spinal cord. Clinical Information. A malignant neoplasm that has spread to the brain from another anatomic site or system. The majority are carcinomas (usually lung or breast carcinomas).
What is metastatic thyroid cancer?
Thyroid cancer metastatic to bone. Clinical Information. Cancer that has spread from the original (primary) tumor to the bone. The spread of a malignant neoplasm from a primary site to the skeletal system. The majority of metastatic neoplasms to the bone are carcinomas.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is C7B in medical terms?
secondary carcinoid tumors ( C7B.-) secondary neuroendocrine tumors ( C7B.-) Cancer that has spread from the original (primary) tumor to the bone. The spread of a malignant neoplasm from a primary site to the skeletal system.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What is a C25.9?
secondary carcinoid tumors ( C 7B.-) secondary neuroendocrine tumors ( C7B.-) Cancer that has spread from the original (primary) tumor to the bone.
What chapter is functional activity?
Functional activity. All neoplasms are classified in this chapter, whether they are functionally active or not. An additional code from Chapter 4 may be used, to identify functional activity associated with any neoplasm. Morphology [Histology]
When will the ICd 10 C79.51 be released?
The 2022 edition of ICD-10-CM C79.51 became effective on October 1, 2021.
What is the ICd 10 code for cerebral meninges?
Secondary malignant neoplasm of cerebral meninges 1 C79.32 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. 2 The 2021 edition of ICD-10-CM C79.32 became effective on October 1, 2020. 3 This is the American ICD-10-CM version of C79.32 - other international versions of ICD-10 C79.32 may differ.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
When will the ICd 10 C79.32 be released?
The 2022 edition of ICD-10-CM C79.32 became effective on October 1, 2021.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is metastasis in cancer?
A tumor that has spread from its original (primary) site of growth to another site, close to or distant from the primary site. Metastasis is characteristic of advanced malignancies, but in rare instances can be seen in neoplasms lacking malignant morphology.
What is a type 1 exclude note?
A type 1 excludes note is a pure excludes. It means "not coded here". A type 1 excludes note indicates that the code excluded should never be used at the same time as C79.9. A type 1 excludes note is for used for when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
What chapter is neoplasms classified in?
All neoplasms are classified in this chapter, whether they are functionally active or not. An additional code from Chapter 4 may be used, to identify functional activity associated with any neoplasm. Morphology [Histology] Chapter 2 classifies neoplasms primarily by site (topography), with broad groupings for behavior, malignant, in situ, benign, ...
When will the ICd 10 C79.9 be released?
The 2022 edition of ICD-10-CM C79.9 became effective on October 1, 2021.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
How long does it take for leptomeningeal metastasis to appear?
The onset of symptoms in most cases ranges from several days to weeks. The clinical manifestations often involve multiple segments of the CNS axis.
Why is leptomeningeal metastasis favored?
The term “leptomeningeal disease” or “leptomeningeal metastases” is favored because it includes malignancies other than carcinoma and excludes dural metastasis. Clinical manifestations. Presentation and course. Most commonly, leptomeningeal metastasis becomes evident late in the course of malignancy, often when metastases are present at other sites.
What are the mechanisms of leptomeningeal metastasis?
Potential mechanisms for the development of leptomeningeal metastasis include hematogenous metastasis directly to the leptomeninges, direct invasion of the meninges from vertebral metastases (especially with lung and breast carcinoma), spread via nerve sheaths (especially with abdominal malignancies), and shedding of cells from solid brain metastases into CSF (especially after surg ical breach of the ventricle at the time of metastasis surgery). Other postulated routes include hematogenous metastasis to the choroid plexus; spread via the perineural, endoneural, and perivascular lymphatics in nerve roots or cranial nerves; and spread via Batson venous plexus.
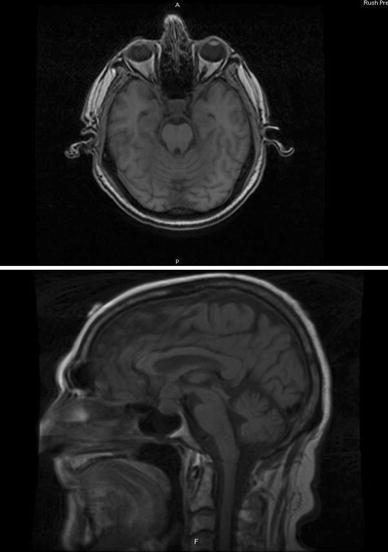
Why do we do MRI before lumbar puncture?
It is desirable to do MRI before lumbar puncture because lumbar puncture can give rise to temporary meningeal enhancement due to arachnoiditis that can be misleading. However, the pattern of enhancement post-lumbar puncture is usually smooth pachymeningeal (not leptomeningeal) enhancement. In patients with suspected leptomeningeal disease, the entire neuraxis should be imaged. The leptomeningeal enhancement can be nodular or scattered over the surface of the brain, spine, or cranial nerves and spinal nerve roots in a “sugar coated” manner as above.
Where is leptomeningeal enhancement?
The leptomeningeal enhancement can be nodular or scattered over the surface of the brain, spine, or cranial nerves and spinal nerve roots in a “sugar coated” manner as above. Leptomeningeal disease (spine MRI) MRI of the spine shows enhancement along the dorsal aspect of the thoracic spinal cord.
How many articles are there in neurology?
Full spectrum of neurology in 1,200 comprehensive articles.
What is the cranial nerve syndrome?
The cranial nerve syndrome involves dysfunction of one or multiple cranial nerves that can lead to visual loss with involvement of cranial nerve II; diplopia with involvement of cranial nerves III, IV, and VI; hearing loss and vertigo with involvement of cranial nerve VII and VIII; and dysphagia and dysarthria with involvement of cranial nerves IX, X, and XII.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is a malignant neoplasm?
Malignant neoplasms of ectopic tissue are to be coded to the site mentioned, e.g., ectopic pancreatic malignant neoplasms are coded to pancreas, unspecified ( C25.9 ). A primary or metastatic malignant neoplasm affecting the brain. Cancer of the brain is usually called a brain tumor. There are two main types.
What chapter is neoplasms classified in?
All neoplasms are classified in this chapter, whether they are functionally active or not. An additional code from Chapter 4 may be used, to identify functional activity associated with any neoplasm. Morphology [Histology] Chapter 2 classifies neoplasms primarily by site (topography), with broad groupings for behavior, malignant, in situ, benign, ...
When will the ICD-10 C71.9 be released?
The 2022 edition of ICD-10-CM C71.9 became effective on October 1, 2021.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What is the name of the cancer that is a rare form of LC?
ALTERNATE NAMES. Leptomeningeal Cancer; Neoplastic Meningitis; Carcinomatous Meningitis; Leptomeningeal Metastasis; Leptomeningeal Carcinoma; Meningeal Metastasis. DESCRIPTION. Leptomeningeal Carcinomatosis (LC) is a rare complication of cancer in which cancerous cells spread to the membranes (meninges) that covers the brain and spinal cord.
What is the diagnosis of LC?
Diagnostic testing: The diagnosis of LC is made with lumbar puncture with positive CSF (cerebral spinal fluid) cytology; and gadolinium enhanced multiplanar MRI of the brain, spinal cord, cauda equina, or subependymal areas.
What is LC in grade 2 brain cancer?
LC in child grade II brain cancers medically equals the criteria in listing 13.13 A 2 if progressive or recurrent following initial antineoplastic therapy.
What is the treatment for LC?
The treatment of LC is symptom-specific and palliative. Most people with LC are treated with surgery, radiation, and chemotherapy. Individuals with this disorder are often prescribed analgesics with opioids, anticonvulsants for seizures, antidepressants, and anxiolytics. SUGGESTED PROGRAMMATIC ASSESSMENT*.
How long does a person with LC live?
LC occurs in approximately 5% of people with cancer and is usually terminal. If left untreated, the median survival is 4-6 weeks; if treated, the median survival is 7 months for people with LCs from the breast, and approximately 4 months for people with LCs from small-cell lung carcinomas and melanomas. TREATMENT.
When does LC meet the criteria in listing 13.27?
LC meets the criteria in listing 13.27 when the primary site is unknown.
Popular Posts:
- 1. icd 10 code for papilledema ou
- 2. icd 10 code for chlamydia trachomatis
- 3. icd-10 code for conjunctivochalasis
- 4. icd 10 code for recurrent small bowl obstruction
- 5. icd 10 code for placenta previa with hemorrhage
- 6. icd 10 code for general pediatric physical with abnormal finding
- 7. icd 10 code for chronic portal vein thrombosis
- 8. icd 10 code for chronic lumbar pain
- 9. icd code for cystitis
- 10. icd-10 code for ventricular escape beats