I44. 1 - Atrioventricular block, second degree | ICD-10-CM.
What is the ICD 10 code for Mobitz type I AV block?
Patient presents to the physician's office after a syncopal episode. An EKG is performed in the office and the patient is diagnosed with a Mobitz type I AV block. What ICD-10-CM code is reported? I44.1
How do you diagnose Mobitz type 1 block?
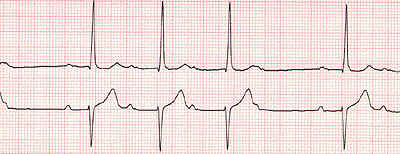
The key to diagnosing Mobitz type I block is looking closely at the PR interval on the ECG strip. In Mobitz I, the sinus node is healthy and fires right on time, so the P waves come at regular intervals.
Is Wenckebach block the same as Mobitz type 1?
Yes, Mobitz type I is also known as Wenckebach block or 2 nd degree heart block type I. All three names refer to the same ECG rhythm and can be used interchangeably. Join millions of students and clinicians who learn by Osmosis! What is the difference between Mobitz I and Mobitz II?
Is syncope a symptom of a Mobitz 1 block?
I44.1 RATIONALE: The syncope is a sign/symptom of the AV block and is not reported. Mobitz I is a second-degree block. Look in theICD-10-CM Alphabetic Index for Mobitz heart block (atrioventricular) or Block, blocked/ atrioventricular/ with/second degree types I and II referring you to I44.1.

What is Mobitz Type 1 heart block?
Mobitz type 1 block is characterized by a gradual prolongation of the PR interval over a few heart cycles until an atrial impulse is completely blocked, which manifests on the ECG as a P-wave not followed by a QRS complex. This cycle repeats itself over and over again, such that every cycle ends with a blocked P-wave.
Is Mobitz Type 1 Wenckebach?
In second-degree atrioventricular nodal block — also known as Wenckebach block or Mobitz Type I AV block — varying failure of conduction through the AV node occurs, such that some P waves may not be followed by a QRS complex. Unlike first-degree AV nodal block, a 1:1 P-wave-to-QRS-complex ratio is not maintained.
Which is another name for Mobitz type I AV block?
There are two types of second-degree atrioventricular blocks: Mobitz type I, also known as Wenckebach and Mobitz type II. This activity examines when this condition should be considered on differential diagnosis and how to properly evaluate for it.
What is ICD-10 code for high grade AV block?
I44. 2 - Atrioventricular block, complete | ICD-10-CM.
What's the difference between Mobitz 1 and Mobitz 2?
Mobitz 1 and 2 are the two forms of second-degree heart block. The difference between them is in mobitz 1 there is a gradual increase in the duration of PR interval until an impulse completely wanes off before reaching the ventricles but in mobitz 2 although the PR interval is prolonged it does not change with time.
What is 1st degree AV block?
First-degree atrioventricular (AV) block is a condition of abnormally slow conduction through the AV node. It is defined by ECG changes that include a PR interval of greater than 0.20 without disruption of atrial to ventricular conduction. This condition is generally asymptomatic and discovered only on routine ECG.
How does a 1st degree AV block differ from a 2nd degree AV block?
This is the mildest type of heart block. Second-degree heart block is classified into two categories: Type I and Type II. In second-degree heart block, the impulses are intermittently blocked. Type I, also called Mobitz Type I or Wenckebach's AV block: This is a less serious form of second-degree heart block.
How common is Mobitz 1?
First degree and Mobitz type 1 heart blocks are uncommon but not rare. It is estimated that 0.5-2% of otherwise healthy adults have these types of heart blocks.
What is Mobitz type 2 AV block?
Mobitz type II second-degree block is an old term, which refers to periodic atrioventricular block with constant PR intervals in the conducted beats. The distinction between type II and type I block is descriptive; of greater importance to the clinician is the anatomic site of the block and the prognosis.
What is the ICD-10 code for AV block?
ICD-10 code I44. 2 for Atrioventricular block, complete is a medical classification as listed by WHO under the range - Diseases of the circulatory system .
What is high grade AV block?
High-grade AV block, also known as advanced heart block, is a form of third-degree heart block. This occurs when AV dissociation is present; however, intermittently some sinus node action potentials (P waves) are randomly conducted to the ventricles.
What is complete AV block?
Complete heart block is the most serious type of AV heart block. It happens when the electrical impulses that tell your heart when to beat don't pass between the top (atria) and bottom chambers (ventricles) of your heart. This can affect the flow of blood to your body and brain.
What is the ICd 10 code for atrioventricular block?
I44.1 is a valid billable ICD-10 diagnosis code for Atrioventricular block, second degree . It is found in the 2021 version of the ICD-10 Clinical Modification (CM) and can be used in all HIPAA-covered transactions from Oct 01, 2020 - Sep 30, 2021 .
Do you include decimal points in ICD-10?
DO NOT include the decimal point when electronically filing claims as it may be rejected. Some clearinghouses may remove it for you but to avoid having a rejected claim due to an invalid ICD-10 code, do not include the decimal point when submitting claims electronically. See also: Block, blocked.
What is Mobitz type 1?
Mobitz type I is a type of 2 nd degree AV block, which refers to an irregular cardiac rhythm (arrhythmia), that reflects a conduction block in the electrical conduction system of the heart. The heart is a muscular organ composed of four chambers: two upper chambers—the right and left atria—, and two lower chambers— the right and left ventricles.
What causes Mobitz block?
Other causes of Mobitz type I block include a heart attack, disorders affecting the heart muscle walls (cardiomyopathies), inflammation of the heart muscle ( myocarditis ), infection of the inner layer of the heart ( endocarditis ), inherited heart defects, infiltrative and autoimmune disorders, and cardiac surgical procedures.
What is the difference between a 1st degree and a 2nd degree AV block?
A 1 st degree AV block is not technically a block, but rather a delay in the conduction of atrial impulses to the ventricles , which results in an extended PR interval. Meanwhile, a 2 nd degree AV block occurs when some of the atrial impulses are fully conducted to the ventricles, whereas others are blocked along the way.
Can Mobitz block cause dizziness?
Some individuals may occasionally feel light-headedness, dizziness, or fatigue when exercising. More rarely, Mobitz type I block may lead to a sudden and temporary loss of consciousness, also known as a syncope, caused by a brief decrease in the oxygen supply to the brain.
Is Mobitz a heart block?
Yes, Mobitz type I is also known as Wenckebach block or 2 nd degree heart block type I. All three names refer to the same ECG rhythm and can be used interchangeably.
Is Mobitz II a good rhythm?
Mobitz I is a benign rhythm that generally reflects a block at the AV node, and typically results in a good prognosis. On the other hand, Mobitz II reflects a block after the AV node, either at the bundle of His or its branches, and often results in a poorer prognosis, as it has a higher risk of progressing to a 3 rd degree AV block.
Does Mobitz I have a sinus node?
In Mobitz I, the sinus node is healthy and fires right on time, so the P waves come at regular intervals. However, atrial impulses travelling through the AV node take longer and longer to conduct at each subsequent impulse, causing a progressive prolongation of the PR interval, until one impulse is completely blocked.
Popular Posts:
- 1. icd 10 code for fx ribs multiple right
- 2. icd 10 code for aftercare following kidney transplant
- 3. icd 10 cm code for uti in pregnancy
- 4. icd 10 code for s/p cardiac arrest
- 5. icd 10 code for renal bruits
- 6. icd 10 diagnosis code for chronic granulomatous disease
- 7. icd 9 code for patellar tendon tear
- 8. icd 10 code for bilateral lower extremity deep venous thrombosis
- 9. icd 10 code for deep vein thrombosis bilateral
- 10. icd 10 cm code for subconjunctival hemorrhage left eye