Z53. 20 - Procedure and treatment not carried out because of patient's decision for unspecified reasons. ICD-10-CM.
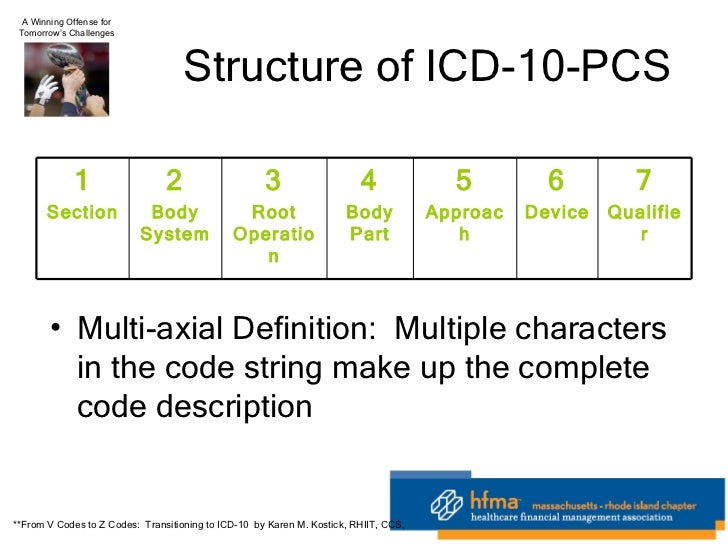
How many codes in ICD 10?
Administrative encounter; Administrative encounter done; Did not attend; Encounter reviewed with preceptor; Medical exam for administrative purposes; Medical examination for administrative purposes done; No show; Patient no show; Review with preceptor done. ICD …
What are the unusual ICD-10 codes?
Oct 01, 2021 · No show Patient no show Review with preceptor done Present On Admission Z02.9 is considered exempt from POA reporting. ICD-10-CM Z02.9 is grouped within Diagnostic Related Group (s) (MS-DRG v39.0): 951 Other factors influencing health status Convert Z02.9 to …
What are the new features of ICD 10?
Oct 01, 2021 · 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code. Z53.9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z53.9 became effective on October 1, 2021. This is the American ICD-10-CM version of Z53.9 - other international versions of ICD-10 Z53.9 may differ.
What are the new ICD 10 codes?
Oct 19, 2021 · The files in the Downloads section below contain information on the ICD-10-CM COVID-19 updates effective with discharges and patient encounters on and after January 1, 2021. The 2021 ICD-10-CM files below contain information on the ICD-10-CM updates for FY 2021. These 2021 ICD-10-CM codes are to be used for discharges occurring from October 1 ...
What is the ICD 10 code for failed outpatient treatment?
Procedure and treatment not carried out, unspecified reason Z53. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z53. 9 became effective on October 1, 2021.
What is Z02 89?
ICD-10 code Z02. 89 for Encounter for other administrative examinations is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is the ICD 10 code for refusal of treatment?
ICD-10-CM Code for Patient's noncompliance with medical treatment and regimen Z91. 1.
What is the ICD-10 diagnosis code for left without being seen?
Z53. 21 is the diagnosis code I dread. When we do our medical charting, it's the code that we use for: “Procedure and treatment not carried out due to patient leaving prior to being seen by health care provider”. In medical slang we say “left without being seen.”Apr 21, 2017
What is diagnosis code Z03 89?
Encounter for observation for other suspected diseases and conditions ruled out. Z03. 89 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
When is Z02 89 used?
Z02. 89 is a billable diagnosis code used to specify a medical diagnosis of encounter for other administrative examinations.
What is the ICD-10 code for non compliant patient?
Patient's noncompliance with other medical treatment and regimen. Z91. 19 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD-10 code for noncompliance?
Z91. 1 - Patient's noncompliance with medical treatment and regimen | ICD-10-CM.
What is the ICD-10 code for History of noncompliance?
ICD-10 code: Z91. 1 Personal history of noncompliance with medical treatment and regimen - gesund.bund.de.
Can you bill an E&M when the patient is not present?
Typically, insurers (including Medicare) will not cover an evaluation and management (E/M) service with a patient's family or caretaker(s) if the patient is not present.Aug 1, 2014
What additional diagnosis code is reported to show that the patient decided not to proceed?
Z53. 20 - Procedure and treatment not carried out because of patient's decision for unspecified reasons | ICD-10-CM.
When do you use 99211?
CPT defines this code as an “office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician.” It further states that the presenting problems are usually minimal, and typically five minutes are spent performing or supervising these services.
What is a Z40-Z53?
Categories Z40-Z53 are intended for use to indicate a reason for care. They may be used for patients who have already been treated for a disease or injury, but who are receiving aftercare or prophylactic care, or care to consolidate the treatment, or to deal with a residual state. Type 2 Excludes.
Why is Z53.20 not carried out?
Z53.20 Procedure and treatment not carried out because of patient's decision for unspecified reasons. Z53.21 Procedure and treatment not carried out due to patient leaving prior to being seen by health care provider. Z53.29 Procedure and treatment not carried out because of patient's decision for other reasons.
Why is there no diagnosis in medical billing?
In many cases, patients come in with symptoms that prompt them to seek medical treatment, yet the physician can make no diagnosis. These cases often result in errors in medical billing coding due to confusion about how to handle the situation. However, in every case, a method exists for proper coding and billing for treatment.
What is the ICD-10 code for a nonspecific condition?
ICD-10 guidelines offer clear specifications on billing codes even when a nonspecific condition presents itself and no diagnosis is forthcoming. While the process of arriving at the correct code may be confusing, getting the coding correct will lead to accurate billing, which translates into timelier payments, happier patients, and avoidance of underpayments. As such, every effort should be made to research and apply the appropriate codes, even in cases where the physician cannot make a diagnosis.
Why do patients leave the office without a diagnosis?
There are many reasons that a patient might report to a physician and leave the office without a diagnosis – maybe the symptoms are nonspecific, or maybe the patient requires a referral to a specialist better suited to make the correct diagnosis. No matter what the reason, coding and billing these cases can be pretty tricky. Medical claims processing is often a complicated and difficult task, and when no diagnosis is reached, properly coding these cases presents a unique challenge.
Why is a symptom not part of a diagnosis?
If the symptom is not part of the diagnosis, it may be listed as part of the history of diagnosis to better explain how the diagnosis was reached, or what obstacles led to difficulties in achieving a diagnosis.
Should symptoms be listed separately in medical coding?
It should be noted that in most cases, listing symptoms in the medical coding where there is a diagnosis is not appropriate. If the symptoms are integral to the diagnosis, the symptom should not be separately listed.
Can a diagnosis be made in a medical billing software?
In this case, no diagnosis can be made and so once again the symptoms presented are instead listed as the codes used in medical billing software. Finally, there are some cases where, even after repeated exams and treatment, defy diagnosis, and a physician may be forced to simply attempt to treat the symptoms or provide palliative care.
Can symptoms disappear before diagnosis?
In many cases, the symptoms were transient and disappear before any diagnosis can be made. In this case, the symptoms themselves are listed in the coding for the billing. In other cases, the symptoms may not immediately lend themselves to a diagnosis; however, rather than returning for a follow-up visit, the patient may elect to find ...
What does "exclude note" mean?
A type 1 excludes note is a pure excludes. It means "not coded here". A type 1 excludes note indicates that the code excluded should never be used at the same time as Z01.84. A type 1 excludes note is for used for when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
What is a Z00-Z99?
Categories Z00-Z99 are provided for occasions when circumstances other than a disease, injury or external cause classifiable to categories A00 -Y89 are recorded as 'diagnoses' or 'problems'. This can arise in two main ways:
What is the ICd 10 code for a procedure?
Z53.20 is a billable diagnosis code used to specify a medical diagnosis of procedure and treatment not carried out because of patient's decision for unspecified reasons. The code Z53.20 is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.#N#The ICD-10-CM code Z53.20 might also be used to specify conditions or terms like 10 year examination not wanted, 15 year examination not wanted, 18 month examination not wanted, 2.5 year examination not wanted, 3.5 year examination not wanted , 4.5 year examination not wanted, etc.#N#The code Z53.20 describes a circumstance which influences the patient's health status but not a current illness or injury. The code is unacceptable as a principal diagnosis.#N#Unspecified diagnosis codes like Z53.20 are acceptable when clinical information is unknown or not available about a particular condition. Although a more specific code is preferable, unspecified codes should be used when such codes most accurately reflect what is known about a patient's condition. Specific diagnosis codes should not be used if not supported by the patient's medical record.
What is an unacceptable principal diagnosis?
Unacceptable principal diagnosis - There are selected codes that describe a circumstance which influences an individual's health status but not a current illness or injury, or codes that are not specific manifestations but may be due to an underlying cause.
When to use Z53.20?
Unspecified diagnosis codes like Z53.20 are acceptable when clinical information is unknown or not available about a particular condition. Although a more specific code is preferable, unspecified codes should be used when such codes most accurately reflect what is known about a patient's condition.
What is the Z53.21 code?
Z53.21 is a billable diagnosis code used to specify a medical diagnosis of procedure and treatment not carried out due to patient leaving prior to being seen by health care provider.
What is an unacceptable principal diagnosis?
Unacceptable principal diagnosis - There are selected codes that describe a circumstance which influences an individual's health status but not a current illness or injury, or codes that are not specific manifestations but may be due to an underlying cause.
Common Circumstances Where No Diagnosis May Be Reached
- There are several circumstances that may arise for a doctor/patient visit that does not result in a diagnosis being reached. For many of these circumstances, there are clear guidelines for medical claims processing on how to code and bill for these services. Preventive care services are often covered by a patient’s insurance and can be billed under the appropriate code for the visit. Thes…
Cases Where An Ill Patient Does Not Receive A Diagnosis
- In many cases, patients come in with symptoms that prompt them to seek medical treatment, yet the physician can make no diagnosis. These cases often result in errors in medical billing coding due to confusion about how to handle the situation. However, in every case, a method exists for proper coding and billingfor treatment. In many cases, where a diagnosis is not immediately abl…
Avoiding Overbilling For Nonspecific Conditions
- ICD-10 guidelines offer clear specifications on billing codes even when a nonspecific condition presents itself and no diagnosis is forthcoming. While the process of arriving at the correct code may be confusing, getting the coding correct will lead to accurate billing, which translates into timelier payments, happier patients, and avoidance of und...
Popular Posts:
- 1. 2018 icd 10 code for immunosuppression
- 2. icd 10 code for steroids
- 3. icd 10 code for migraines wiothout aura
- 4. icd-10 code for migraine without aura
- 5. icd 10 code for skin abrasion unspecified site
- 6. icd-10-cm code for small bowel obstruction
- 7. icd 10 code for pertoneal biopsy
- 8. icd 10 code for stepped on nail
- 9. icd 10 code for nelsons syndrom
- 10. icd 9 code for flexion contracture