Encounter for screening for malignant neoplasm of colon. Z12.11 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2019 edition of ICD-10-CM Z12.11 became effective on October 1, 2018.
Two Sets of Procedure Codes Used for Screening Colonoscopy:
| Common colorectal screening diagnosis codes | |
|---|---|
| ICD-10-CM | Description |
| Z12.11 | Encounter for screening for malignant neoplasm of colon |
| Z80.0 | Family history of malignant neoplasm of digestive organs |
| Z86.010 | Personal history of colonic polyps |
Apr 20, 2022
What are the new ICD 10 codes?
The new codes are for describing the infusion of tixagevimab and cilgavimab monoclonal antibody (code XW023X7), and the infusion of other new technology monoclonal antibody (code XW023Y7).
What is the longest ICD 10 code?
What is the ICD 10 code for long term use of anticoagulants? Z79.01. What is the ICD 10 code for medication monitoring? Z51.81. How do you code an eye exam with Plaquenil? Here’s the coding for a patient taking Plaquenil for RA:Report M06. 08 for RA, other, or M06. Report Z79. 899 for Plaquenil use for RA.Always report both.
Where can one find ICD 10 diagnosis codes?
Search the full ICD-10 catalog by:
- Code
- Code Descriptions
- Clinical Terms or Synonyms
What is the ICD 10 code for short bowel syndrome?
Clozapine is classified as an atypical antipsychotic drug because it binds to serotonin as well as dopamine receptors. Clozapine is an antagonist at the 5-HT 2A subunit of the serotonin receptor, putatively improving depression, anxiety, and the negative cognitive symptoms associated with schizophrenia.
What is the ICD-10 code for colon?
Malignant neoplasm of colon, unspecified C18. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C18. 9 became effective on October 1, 2021.
What is a Z12 11?
Z12. 11 encounter for screening for malignant neoplasm of colon.
What is the difference between 45378 and 45380?
A family of CPT codes applies to colonoscopy. For example, code 45378 applies to a colonoscopy in which no polyp is detected, while codes 45380-45385 apply to colonoscopy that involves an intervention (e.g., 45385 is the code for colonoscopy with polypectomy.)
What is the ICD-10 code for sigmoid colon mass?
C18. 7 - Malignant neoplasm of sigmoid colon | ICD-10-CM.
What does code Z12 31 mean?
For example, Z12. 31 (Encounter for screening mammogram for malignant neoplasm of breast) is the correct code to use when you are ordering a routine mammogram for a patient.
What is code Z12 39?
ICD-10 code Z12. 39 for Encounter for other screening for malignant neoplasm of breast is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is the difference between 45380 and 45385?
45380—Colonoscopy, with biopsy, single or multiple. Hint: The physician may use the words “biopsy forceps,” or “Jumbo forceps.” Fee amount $468.96. 45385—Colonoscopy, with removal of tumor(s), polyp(s), lesion(s) by snare technique.
What is the difference between CPT 45380 and 45385?
The NCCI PTP edit with column one CPT code 45385 (Flexible colonoscopy with removal of tumor(s), polyp(s), or lesion(s) by snare technique) and column two CPT code 45380 (Flexible colonoscopy with single or multiple biopsies) is often bypassed by utilizing modifier 59.
What is the diagnosis code for routine colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code V76. 51 (Special screening for malignant neoplasm of the colon).
What is K63 89 diagnosis?
K63. 89 - Other Specified Diseases of Intestine [Internet]. In: ICD-10-CM.
What is diagnosis code z80 9?
9: Family history of malignant neoplasm, unspecified.
What is mass in colon?
Colon cancer is a malignant (cancerous) tumor that grows in the wall of the colon. Most colon tumors begin when normal tissue in the colon wall forms an adenomatous polyp, or pre-cancerous growth, that comes out of the colon wall. As this polyp grows larger, the tumor forms.
What is the code for inflammatory colon polyps?
Codes for inflammatory colon polyps, found in category K51, include a description of complications: K51.40 Inflammatory polyps of colon without complications. K51.411 Inflammatory polyps of colon with rectal bleeding. K51.412 Inflammatory polyps of colon with intestinal obstruction.
Is colon cancer benign?
Print Post. Colorectal cancer typically develops from colon polyps, which are abnormal growths of tissue (neoplasms). Most polyps are benign, but may become cancerous. When selecting an ICD-10 diagnosis code for polyp (s) of the colon, you will need to know the precise location of the polyp (s) and the type of polyp (e.g., benign, inflammatory, ...
What is the code for colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code Z12.11 ( encounter for screening for malignant neoplasm of the colon ).
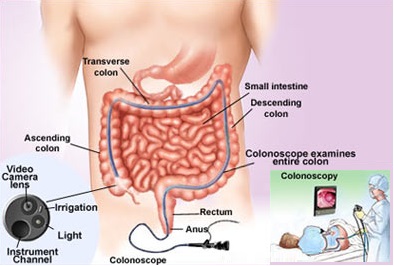
What is a colonoscopy screening?
As such, “screening” describes a colonoscopy that is routinely performed on an asymptomatic person for the purpose of testing for the presence of colorectal cancer or colorectal polyps. Whether a polyp or cancer is ultimately found does not ...
What are the global periods for colonoscopy?
Typically, procedure codes with 0, 10 or 90-day global periods include pre-work, intraoperative work, and post-operative work in the Relative Value Units (RVUs) assigned . As a result, CMS’ policy does not allow for payment of an Evaluation and Management (E/M) service prior to a screening colonoscopy. In 2005, the Medicare carrier in Rhode Island explained the policy this way:
Why is diagnosis code ordering important?
Diagnosis Code Ordering is Important for a Screening Procedure turned Diagnostic. When the intent of a visit is screening, and findings result in a diagnostic or therapeutic service, the ordering of the diagnosis codes can affect how payers process the claim.
Is colonoscopy a first dollar service?
Screening colonoscopy is a service with first dollar coverage. A screening test with an A or B rating from the US Preventive Services Task Force, should have no patient due amount, since the Affordable Care Act (ACA) was passed.
Can a patient have a colonoscopy?
The patient has never had a screening colonoscopy. The patient has no history of polyps and none of the patient’s siblings, parents or children has a history of polyps or colon cancer. The patient is eligible for a screening colonoscopy. Reportable procedure and diagnoses include:
Does Medicare waive co-pay for colonoscopy?
However, diagnostic colonoscopy is a test performed as a result of an abnormal finding, sign or symptom. Medicare does not waive the co-pay and deductible when the intent of the visit is to perform a diagnostic colonoscopy.

Benign Colon Polyps
Codes for benign adenomatous polyp of the colon are found in the neoplasm chapter of ICD-10-CM, by location: Example: A 68-year-old, asymptomatic patient undergoes screening colonoscopy. The physician finds and snares a tubular adenoma in the cecum. Because this is a screening, the primary diagnosis is Z12.…
Inflammatory Polyps
- Codes for inflammatory colon polyps, found in category K51, include a description of complications: Per ICD-10 guidelines, you should use an additionalcode with category K51 to identify manifestations (e.g., pyoderma gangrenosum).
Other Polyps
- Polyps of the colon not documented as adenomatous, benign, or inflammatory are reported using K63.5 Polyp of colon. If a colon polyp is specified as hyperplastic, assign K63.5 even if greater specificity is provided regarding the location, per Coding Clinic for ICD-10-CM and ICD-10-PCS (Second Quarter 2015, pages 14-15). The ICD-10 code for rectal polyp is K62.1 Rectal polyp…
Malignant Neoplasms
- For malignant neoplasm(s) of the colon and rectum, refer to ICD-10 categories C18-C20. Example: A 70-year-old patient with a family history of colon cancer complains of abdominal pain and rectal bleeding. During colonoscopy, the physician finds a mass at the hepatic flexure, which pathology confirms as malignant. The primary diagnosis is cancer of ...
Popular Posts:
- 1. icd 10 code for pain rt wrist
- 2. icd 10 code for joint pain other
- 3. icd 9 code for stasis ulcer of leg
- 4. what is the icd-10 cpt code for eeg 13.9
- 5. icd-10-cm code for vitiligo
- 6. icd 10 code for testing for folic acid
- 7. icd code for history of breast cancer
- 8. icd 10 code for periventricular leukomalacia
- 9. icd 10 code for nodule left breast
- 10. icd 10 code for interstitial cystitis?trackid=sp-006