ICD-10 Code for Gastrointestinal hemorrhage, unspecified- K92. 2- Codify by AAPC.
Where can one find ICD 10 diagnosis codes?
Search the full ICD-10 catalog by:
- Code
- Code Descriptions
- Clinical Terms or Synonyms
What is the ICD 10 code for GERD?
Gastro-esophageal reflux disease without esophagitis K21. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2020 edition of ICD - 10 -CM K21. 9 became effective on October 1, 2019.
What is the ICD 10 code for GI bleed?
- K20.0, Eosinophilic esophagitis,
- K20.8, Other esophagitis,
- K20.9, Esophagitis, unspecified.
What is the ICD 10 for GERD?
Gastro-esophageal reflux disease with esophagitis. K21.0 is a valid billable ICD-10 diagnosis code for Gastro-esophageal reflux disease with esophagitis. It is found in the 2019 version of the ICD-10 Clinical Modification (CM) and can be used in all HIPAA-covered transactions from Oct 01, 2018 – Sep 30, 2019.
What is the ICD-10 code for gastrointestinal bleeding?
ICD-10 code: K92. 2 Gastrointestinal haemorrhage, unspecified.
What is gastrointestinal hemorrhage unspecified?
Gastrointestinal (GI) bleeding is a symptom of a disorder in your digestive tract. The blood often appears in stool or vomit but isn't always visible, though it may cause the stool to look black or tarry. The level of bleeding can range from mild to severe and can be life-threatening.
What is the CPT code for GI bleed?
2 - Gastrointestinal hemorrhage, unspecified.
What does Melena K92 1 mean?
melena (K92.1) neonatal rectal hemorrhage (P54.2)
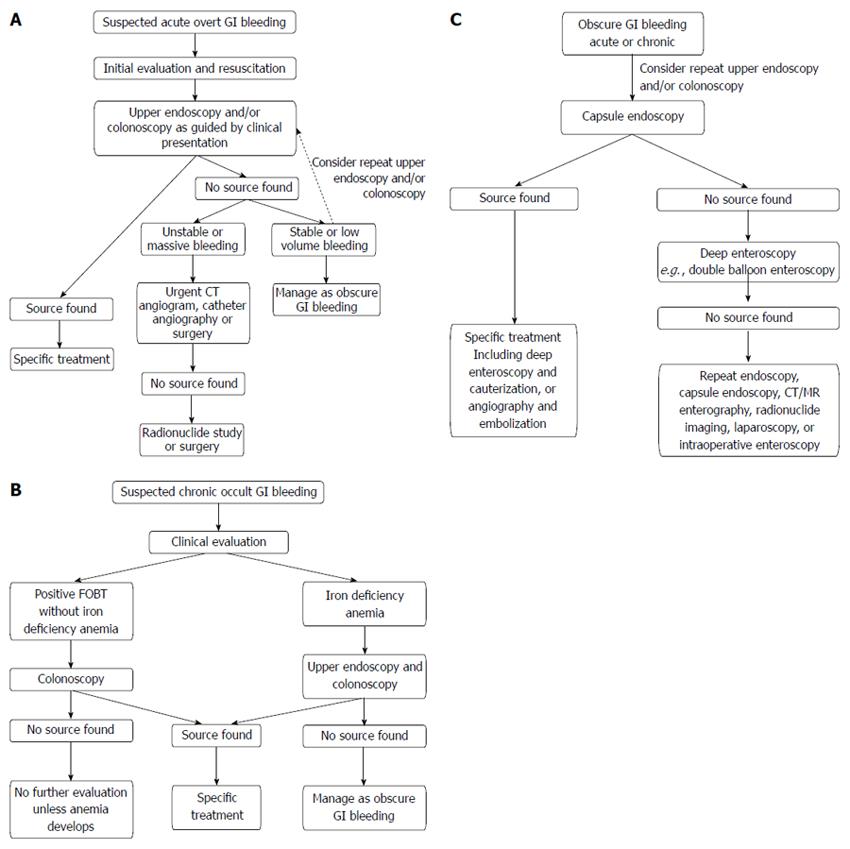
How is gastrointestinal bleeding diagnosed?
An endoscopy procedure may help your doctor see if and where you have GI bleeding and the bleeding's cause. Doctors most often use upper GI endoscopy and colonoscopy to test for acute GI bleeding in the upper and lower GI tracts. Upper GI endoscopy.
What causes gastrointestinal bleeding?
There are many possible causes of GI bleeding, including hemorrhoids, peptic ulcers, tears or inflammation in the esophagus, diverticulosis and diverticulitis, ulcerative colitis and Crohn's disease, colonic polyps, or cancer in the colon, stomach or esophagus.
What does CPT code 43239 mean?
CPT® Code 43239 in section: Esophagogastroduodenoscopy.
What is the ICD 10 code for Hematemesis?
K92.0K92. 0 Hematemesis - ICD-10-CM Diagnosis Codes.
When do you use CPT code 45382?
CPT® Code 45382 - Endoscopy Procedures on the Rectum - Codify by AAPC.
What is melena diagnosis?
Melena refers to black, tar-like, sticky stools and usually results from upper gastrointestinal bleeding. The source of bleeding can come from damage to the lining of the GI tract, breakage of swollen blood vessels, or other conditions that prolong bleeding such as hemophilia.
What is occult blood in stool test?
Overview. The fecal occult blood test (FOBT) is a lab test used to check stool samples for hidden (occult) blood. Occult blood in the stool may indicate colon cancer or polyps in the colon or rectum — though not all cancers or polyps bleed.
What is Melaena stool?
Melena refers to black tarry stools, which usually occurs as a result of upper gastrointestinal bleeding. It has a characteristic tarry colour and offensive smell, and is often difficult to flush away, which is due to the alteration and degradation of blood by intestinal enzymes.
Is gastrointestinal bleeding serious?
GI bleeding is a serious symptom that requires prompt medical treatment. From tears in the organs in the digestive tract to inflammatory conditions, these causes often require examination by a doctor to diagnose and treat. Left untreated, they may result in serious complications, including heart attack and shock.
Does gastrointestinal bleeding go away?
Often, GI bleeding stops on its own. If it doesn't, treatment depends on where the bleed is from. In many cases, medication or a procedure to control the bleeding can be given during some tests.
How do you stop gastrointestinal bleeding?
How do doctors treat GI bleeding?inject medicines into the bleeding site.treat the bleeding site and surrounding tissue with a heat probe, an electric current, or a laser.close affected blood vessels with a band or clip.
What medication can cause gastrointestinal bleeding?
Drugs that can lead to gastrointestinal bleeding include non-steroidal anti-inflammatory drugs (NSAIDs) like diclofenac and ibuprofen, platelet inhibitors such as acetylsalicylic acid (ASS), clopidogrel and prasugrel, as well as anticoagulants like vitamin-K antagonists, heparin or direct oral anticoagulants (DOAKs).
What does "bleeding" mean in medical terms?
Escape of blood from the vessels; bleeding.
What does it mean when you bleed?
Bleeding is the loss of blood. It can happen inside or outside the body. Bleeding can be a reaction to a cut or other wound. It can also result from an injury to internal organs.there are many situations in which you might bleed. A bruise is bleeding under the skin. Some strokes are caused by bleeding in the brain. Other bleeding, such as gastrointestinal bleeding, coughing up blood, or vaginal bleeding, can be a symptom of a disease.normally, when you bleed, your blood forms clots to stop the bleeding. Severe bleeding may require first aid or a trip to the emergency room. If you have a bleeding disorder, your blood does not form clots normally.
When will the ICd 10-CM R58 be released?
The 2022 edition of ICD-10-CM R58 became effective on October 1, 2021.
What is the code for GI bleeding?
Another twist is that Coding Clinic, Second Quarter 2008, page 15, points out Inclusion Terms listed in the Tabular also act as nonessential modifiers, stating GI bleeding due to acute ischemic colitis would be reported with one code, 557.0, Acute vascular insufficiency of intestine. The term hemorrhagic is an Inclusion Term listed under code 557, indicating hemorrhage, is an integral part of this disease process. An additional code to identify GI bleeding is not assigned.
What is the thought process involved in coding for conditions associated with gastrointestinal bleeding?
Examination of the thought process involved in code selection for conditions associated with gastrointestinal bleeding requires knowledge to navigate the twists and turns through coding conventions, guidelines and Coding Clinic advice, as well as the ability to decipher “clinical speak” into “code speak.” On top of everything else, a coder is always focused on the end goal of reporting an accurate account of the patient condition and the care provided. It is like working a bouncing pinball down the table for the highest score.
What is a nonessential modifier?
Nonessential modifiers throw a couple twists into the code selection process. They are supplementary terms, enclosed in parentheses, found in both the Index and Tabular. The presence or absence of these terms in physician documentation has no impact on the code, but add to the thought process in determining the need for additional codes.
What is the default code for anemia?
Assign the default code, 280.0 Anemia secondary to blood loss in the absence of documentation on the acuity of blood loss anemia.
What is the code for acute and chronic blood loss anemia?
If the clinical picture and documentation identify the diagnosis of acute and chronic blood loss anemia, it is appropriate to code both 285.1 Acute blood loss anemia and 280.0 Chronic blood loss anemia.
Is GI bleeding slow or fast?
GI bleeding can be grouped into what is known as “fast bleed” and “slow bleed.” Using this concept, fast bleed can usually point to an acute blood loss anemia, where as a slow bleed usually points to an intermittent or a chronic blood loss anemia. It is possible for a slow bleed to develop into a fast bleed, or both conditions can exist in the same patient at the same time but at different sites. It is possible for a patient to have chronic blood loss anemia and acute blood loss anemia at the same time
Is there a causal relationship between hemorrhoids and rectal bleeding?
In the setting of rectal bleeding with hemorrhoids, without physician documentation of a causal relationship between the hemorrhoids and rectal bleeding, Coding Clinic, Third Quarter 2005, page 17, states to query the physician for clarification as to whether the hemorrhoids are the source of the bleed or an incidental finding.

Popular Posts:
- 1. icd 10 code for ear block
- 2. icd 10 code for bilateral blurred vision
- 3. icd 10 code for resect of third and fourth metatarsal heads
- 4. icd 10 code for posterior cervical adenopathy
- 5. icd-10 code for delirium due to unknown physiological condition
- 6. icd-10 code for coombs positive
- 7. icd-10 code for esophageal stricture
- 8. icd 10 code for severe bipolar disorder, in manic state, without psychosis
- 9. icd code for croup
- 10. icd 10 code for bilateral lower extremity paresis