Psychotic disorder with delusions due to known physiological condition. F06. 2 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD 10 diagnosis code for?
The ICD-10-CM is a catalog of diagnosis codes used by medical professionals for medical coding and reporting in health care settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates.
Should new ICD-10 code reference puerperal psychosis?
F53.1 is a valid billable ICD-10 diagnosis code for Puerperal psychosis . It is found in the 2021 version of the ICD-10 Clinical Modification (CM) and can be used in all HIPAA-covered transactions from Oct 01, 2020 - Sep 30, 2021 .
What is the ICD 10 code for Parkinsons Disease?
Parkinson's disease
- Tabular List of Diseases and Injuries. The Tabular List of Diseases and Injuries is a list of ICD-10 codes, organized "head to toe" into chapters and sections with coding notes ...
- Index to Diseases and Injuries. ...
- Approximate Synonyms
- Clinical Information
- Convert G20 to ICD-9 Code. ...
What is unspecified non organic psychosis?
Unspecified nonorganic psychosis. (Unspecified nonorganic psychosis ) Disease of males and females from the section "Schizophrenia, schizotypal and delusional disorders". Causes not a significant loss of workdays. May be the cause of death. 448 751 people were diagnosed with Unspecified nonorganic psychosis.
What is the ICD-10 code for unspecified psychosis?
ICD-10 code F29 for Unspecified psychosis not due to a substance or known physiological condition is a medical classification as listed by WHO under the range - Mental, Behavioral and Neurodevelopmental disorders .
What is the diagnosis code for psychosis?
psychosis, psychogenic (F23. 3)
What is psychosis F29?
F29 - Unspecified psychosis not due to a substance or known physiological condition.
What is the ICD-10 code for delusional disorder?
8 Other persistent delusional disorders. Disorders in which the delusion or delusions are accompanied by persistent hallucinatory voices or by schizophrenic symptoms that do not justify a diagnosis of schizophrenia (F20.
Is unspecified psychosis a diagnosis?
Unspecified psychosis, defined with the F29 code in the International Classification of Diseases (ICD) 10th version is commonly used if there is inadequate information to make the diagnosis of a specific psychotic disorder.
What does psychosis mean?
During a period of psychosis, a person's thoughts and perceptions are disturbed and the individual may have difficulty understanding what is real and what is not. Symptoms of psychosis include delusions (false beliefs) and hallucinations (seeing or hearing things that others do not see or hear).
What is an acute psychosis?
What is Acute Psychosis. Tab 1 Content. Also known as Brief Psychotic Disorder, this is an acute mental health condition when there is a loss of contact with reality. This is characteristised by one or more of following features. A reduced level of social functioning.
What is the ICD 10 code for dementia with psychosis?
Unspecified dementia with behavioral disturbance The 2022 edition of ICD-10-CM F03. 91 became effective on October 1, 2021.
What causes unspecified psychosis?
Psychosis is a symptom, not an illness. It can be triggered by a mental illness, a physical injury or illness, substance abuse, or extreme stress or trauma. Psychotic disorders, like schizophrenia, involve psychosis that usually affects you for the first time in the late teen years or early adulthood.
How do you code delusional disorder?
F22 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM F22 became effective on October 1, 2021.
What is psychogenic paranoid psychosis?
Psychogenic paranoid psychosis was defined in 1916 by A Wimmer, based on Jaspers' concept of reaction (Jaspers, 1962) as a “group of clinically independent psychoses, with primary characteristic indicating that its onset (generally based on a con- stitutional predisposition) is provoked by mental traumas, in such a way ...
Is delusional disorder the same as schizophrenia?
Delusional disorder is distinguished from schizophrenia by the presence of delusions without any of the other symptoms of psychosis (for example, hallucinations, disorganized speech, or disorganized behavior).
What are the symptoms of Parkinson's disease?
The early stages of PD include the following signs and symptoms: Slight shaking of a finger, hand, leg, chin, or lip. Stiffness or difficulty walking. Difficulty getting out of a chair.
What is the PD G20 code?
With PD G20 code, you will be coding associated signs and symptoms or those complications not necessarily inherent to the disease. Most of these complications will be found in Chapter 18, as signs and/or symptoms.
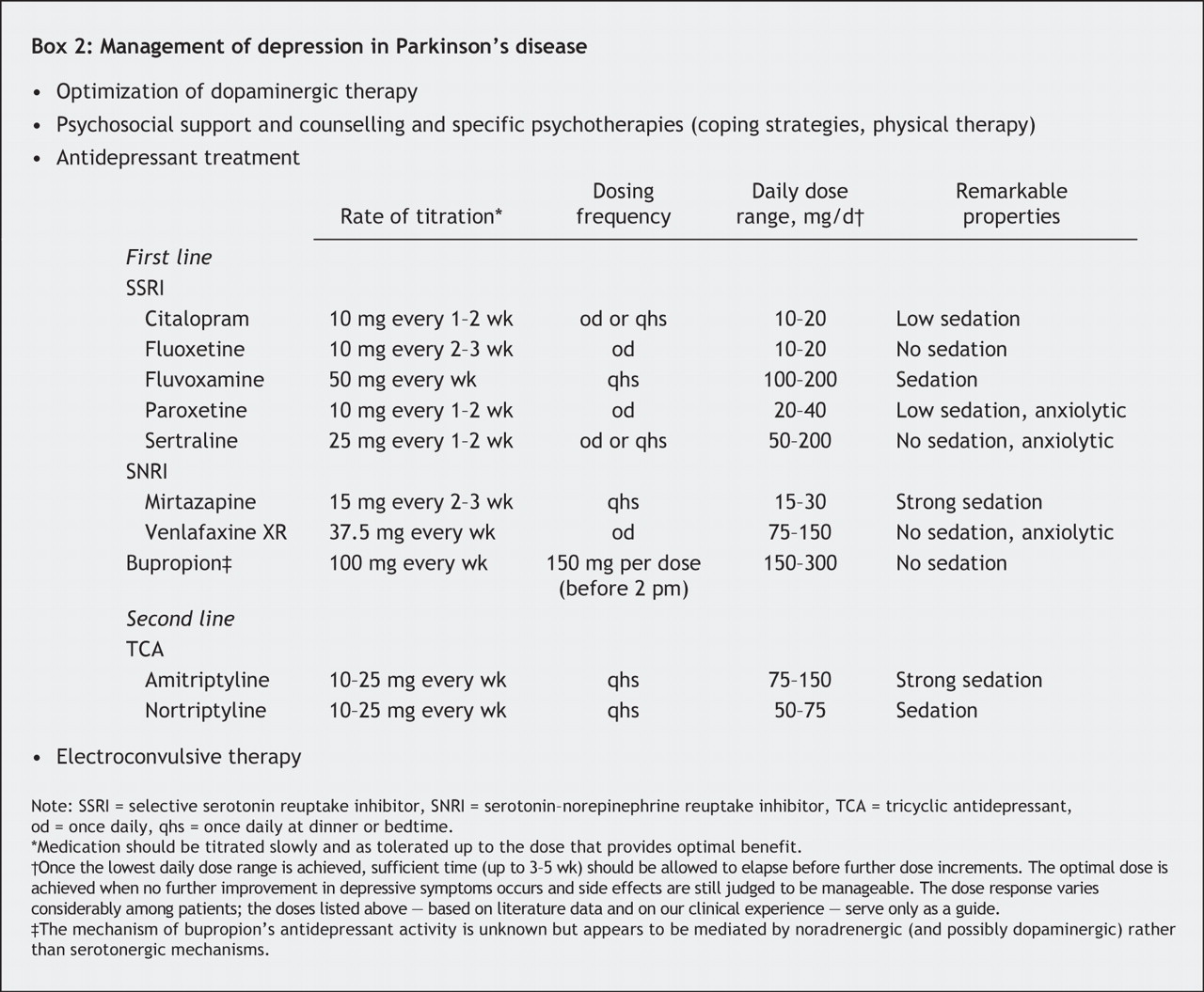
What is the third category of medication for PD?
The third category of drugs prescribed for PD includes medications that help control the non-motor symptoms of the disease ; that is, the symptoms that don't affect movement. For example, people with PD-related depression may be prescribed antidepressants.
How many people are affected by Parkinson's disease?
As a neurodegenerative disease of the brain, which impacts an individual’s motor function, Parkinson’s Disease (PD) is the most common neurological disorder, affecting approximately one million people in the United Status. It is estimated that approximately 60,000 Americans are diagnosed with PD each year, and this number does not reflect ...
What is the second category of PD drugs?
The second category of PD drugs affects other neurotransmitters in the body in order to ease some of the symptoms of the disease. For example, anticholinergic drugs interfere with production or uptake of the neurotransmitter acetylcholine. These can be effective in reducing tremors.
What is Parkinson's disease?
Parkinson's disease is a disorder that affects nerve cells, or neurons, in a part of the brain that controls muscle movement. In parkinson's, neurons that make a chemical called dopamine die or do not work properly. Dopamine normally sends signals that help coordinate your movements.
How old do you have to be to get Parkinson's?
They may also have problems such as depression, sleep problems or trouble chewing, swallowing or speaking. Parkinson's usually begins around age 60, but it can start earlier.
What does the title of a manifestation code mean?
In most cases the manifestation codes will have in the code title, "in diseases classified elsewhere.". Codes with this title are a component of the etiology/manifestation convention. The code title indicates that it is a manifestation code.
What is neurocognitive disorder?
Major neurocognitive disorder in other diseases classified elsewhere with aggressive behavior. Major neurocognitive disorder in other diseases classified elsewhere with combative behavior. Major neurocognitive disorder in other diseases classified elsewhere with violent behavior.
What are the main features of psychosis?
With regard to the clinical definition of the main features of psychosis, which include hallucinations, illusions, and delusions , current ICD-10 guidelines define hallucinations as a disorder characterised by a false sensory perception in the absence of an external stimulus, whereas an illusion is regarded as a misperception of an externally present stimulus. In contrast to classical hallucinations and illusions, delusions are a false interpretation of the experienced misperceptions, often involving topics of persecution, imposters, or grandiosity. Some specific forms of delusions such as the Cotard syndrome (implying nihilistic delusions, hypochondriacal delusions, and delusions of immortality) [ 10 – 12 ], Capgras syndrome (including having the conviction that a family member or friend has been replaced by another), and Othello syndrome (being described as a delusional jealousy) have further been named [ 13, 14 ], the latter showing an association with dopamine agonist therapy and an improvement after its reduction. The current diagnostic criteria from ICD-10 based guidelines for acute and transient psychosis are shown in Box 1; other definitions of psychosis falling under the term of schizoaffective disorders will not be further developed in this review.
How long does psychosis last?
If isolated visual hallucinations manifest independently or before the onset of “classical” PD psychosis, which is defined as lasting for over 1 month, it has been described as mostly resulting from medication [ 56 ]. An acute setting with sudden onset of psychotic symptoms must be regarded as an emergency situation [ 57 ]. Apart from recent changes in PD medication and acute intoxications associated with dehydration or other metabolic disorders, less frequent differential diagnosis such as cerebral infarction, intracranial haemorrhage, or CNS infections needs to be addressed. It is well known that some specific medical comorbidities can acutely trigger a psychotic episode or influence the severity of its symptoms [ 3 ], including infections, dehydration, sleep deprivation, irregular nutrition, psychosocial stress, deprivation or overload of sensory inputs, operations, metabolic alterations, dopaminergic drugs, and some other not antiparkinsonian drugs such as beta-blockers or corticosteroids. Under benzodiazepines a paradoxical reaction with restlessness, excitation, and euphoria may occur.
Is pimavanserin a dopaminergic agonist?
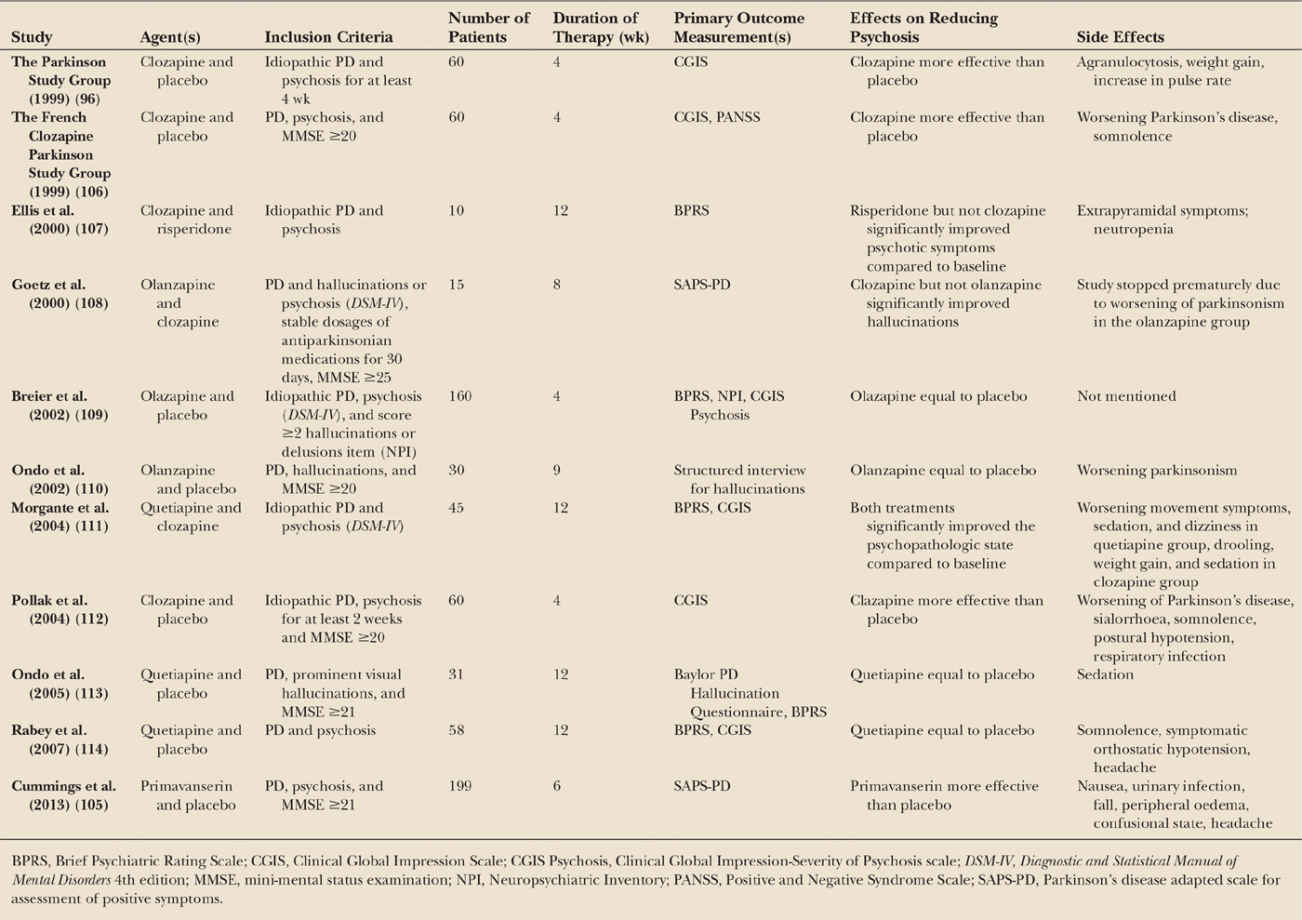
Pimavanserin, a selective 5-HT2A inverse agonist without dopaminergic, adrenergic, histaminergic, or muscarinic effect [ 141 ], has been approved by the FDA [ 142] in September 2014 and has shown to be effective and safe in the treatment of PD psychosis, reducing hallucinations and delusions without affecting motor function [ 143, 144 ], which is a commonly observed drawback of most antipsychotic drugs due to dopamine antagonism. Recent studies have shown the potential of this drug to improve psychotic symptoms among PD patients [ 144, 145 ]. Results showed a significant improvement in measures of psychosis in PD patients without impairing motor function in one study by Meltzer et al. [ 145] and a statistically significant decrease in SAPS-PD scores in a bigger cohort of 199 PD patients in a randomized, double-blind, placebo-controlled phase 3 trial by Cummings et al. [ 144 ]. But pimavanserin and commonly used antipsychotics have up to now not been systematically compared.
Is Clozapine a psychotropic drug?
Clozapine is an atypical antipsychotic whose mechanism of action is only partially understood, being thought to mainly act as an antagonist of dopamine D2 receptors and serotonin 2A receptors. It was first produced in 1958 and sold commercially after 1972. A double-blind, placebo-controlled study on clozapine for the treatment of drug-induced psychosis in PD (PSYCLOPS trial) showed an effectiveness of low-dose clozapine without worsening of motor function and response maintenance over at least 4 months in PD patients with psychosis [ 126 ]. A further double-blind, placebo-controlled study by Pollak et al. could find a statistically significant improvement in psychosis scores when compared to placebo, without significant motor function worsening, when using a low dose of clozapine of 50 mg/day. They also found wearing-off of the effect after discontinuation of the therapy [ 127 ]. These studies support the effectiveness of low-dose clozapine for the management of psychosis in PD.
Is PD psychosis intrinsic or extrinsic?
The pathophysiological processes underlying PD psychosis can be subdivided into intrinsic (neurotransmitter-dysfunction related and thus not externally induced) and extrinsic (drug-related and thus a direct result of the use of pharmacological agents). While intrinsic PD psychosis is thought to be caused by alterations in dopamine, serotonin, and acetylcholine systems involving subcortical projections as well as synaptic and neuronal changes in limbic and cortical structures [ 76 ], extrinsic PD mainly involves dopaminergic or anticholinergic therapies, especially dopamine agonists [ 35, 72 ].
Is psychosis a nonmotor disorder?
Although psychosis was thoroughly studied in recent years after being identified as one of the most relevant nonmotor features in PD, standardized guidelines for the management of PD psychosis are not available. Interestingly, psychosis, being one of the hallmarks of psychiatric illnesses such as schizophrenia with patients typically presenting with auditory features [ 21 ], presents rather differently in PD patients, where visual hallucinations clearly predominate, implicating a potentially different entity and thus underlying pathophysiological mechanism, further challenging the actual use of the same treatment options for both. In addition, current hypotheses on the underlying pathophysiological mechanisms including neurotransmitter dysregulation, structural/functional brain imaging abnormalities, and blood and CSF based biochemical measurements are sparse and inconsistent, supporting the lack of knowledge and the need of further investigation in order to potentially develop target oriented drugs in the nearer future. Currently undergoing studies on novel drugs for PD psychosis are expected to produce results in due time; ideas of further intervention strategies such as deep brain stimulation or stem cell therapy are being addressed for other causes of psychosis and could, if efficient, pose further options in the future. For now it remains clear that much more effort needs to be put into understanding this condition.
Popular Posts:
- 1. icd 10 code for dysphagia due to old cva
- 2. icd 10 code for failed kidney transplant
- 3. icd 9 code for lumbar spine sprain strain
- 4. icd-10 code for picc line placement
- 5. icd 10 code for female infertility due to postoperative peritubal adhesions
- 6. icd 10 code for right total knee infection
- 7. icd 10 code for history of hartmann reversal
- 8. icd 10 code for decreased urine stream
- 9. icd 10 cm code for colostomy problem
- 10. icd-10 code for difficulty walking