89.
Full
AnswerHow many codes in ICD 10?
- ICD-10 codes were developed by the World Health Organization (WHO) External file_external .
- ICD-10-CM codes were developed and are maintained by CDC’s National Center for Health Statistics under authorization by the WHO.
- ICD-10-PCS codes External file_external were developed and are maintained by Centers for Medicare and Medicaid Services. ...
What are the new ICD 10 codes?
The new codes are for describing the infusion of tixagevimab and cilgavimab monoclonal antibody (code XW023X7), and the infusion of other new technology monoclonal antibody (code XW023Y7).
What is the purpose of ICD 10?
Why ICD-10 codes are important
- The ICD-10 code system offers accurate and up-to-date procedure codes to improve health care cost and ensure fair reimbursement policies. ...
- ICD-10-CM has been adopted internationally to facilitate implementation of quality health care as well as its comparison on a global scale.
- Compared to the previous version (i.e. ...
What is the ICD 10 code for pre op clearance?
What is the ICD 10 code for preoperative clearance? Z01.818 Most pre-op exams will be coded with Z01. 818. The ICD-10 instructions say to use the preprocedural diagnosis code first, and then the reason for the surgery and any additional findings. Evaluations before surgery are reimbursable services. Is deconditioning a diagnosis?
How do you code a pre-op physical?
Most pre-op exams will be coded with Z01. 818. The ICD-10 instructions say to use the preprocedural diagnosis code first, and then the reason for the surgery and any additional findings. Evaluations before surgery are reimbursable services.
What is the ICD-10 code for pre-op clearance?
A preoperative examination to clear the patient for surgery is part of the global surgical package, and should not be reported separately. You should report the appropriate ICD-10 code for preoperative clearance (i.e., Z01. 810 – Z01.
What is the diagnosis code for physical therapy?
Common ICD-10 codes for physical therapyCodeShort DescriptorM54.2CervicalgiaM25.511Pain in right shoulderM25.561Pain in right kneeM25.512Pain in left shoulder6 more rows
What is the CPT code for a pre-op visit?
When the surgeon sees the patient the day of surgery prior to the operation that visit is not billable. This is because the preoperative time of that visit has already been valued in the 90-day global code (CPT 27447) as part of the pre-time package.
Can you bill for a pre op?
Preoperative examinations may be billed by using an appropriate CPT code (e.g., new patient, established patient, or consultation). Such non-global preoperative examinations are payable if they are medically necessary and meet the documentation and other requirements for the service billed.
What is the ICD-10 diagnosis code for medical clearance?
ICD-10 Code for Encounter for issue of other medical certificate- Z02. 79- Codify by AAPC.
Can physical therapists assign ICD-10 codes?
Just as in ICD-9, every claim form that is submitted for a patient treatment must have codes that support the treatment. So, yes, there will be ICD-10 codes for every encounter. Typically, during the evaluation, the therapist identifies the codes.
Can physical therapists add ICD-10 codes?
On October 1, 2015, physical therapists and other HIPAA-covered providers transitioned from ICD-9 to the diagnosis code set known as the Tenth Revision to the International Classification of Diseases (ICD-10).
What are ICD-10 codes occupational therapy?
Commonly-Used OT ICD-10 CodesR63.3 — Feeding difficulties.G54.0 – Brachial Plexus disorders.R62.0 — Delayed milestones in childhood.G82.20 — Paraplegia unspecified.R27.0 — Ataxia, unspecified.F82 — Specific developmental disorder of motor function.M62.81 — Muscle weakness (generalized)More items...
What is preoperative diagnosis?
Definition: The Preoperative Diagnosis Section records the surgical diagnosis or diagnoses that are assigned to the patient before the surgical procedure, and is the reason for the surgery. The Preoperative Diagnosis is, in the opinion of the surgeon, the diagnosis that will be confirmed during surgery.
Does Medicare cover pre-op physicals?
Medical preoperative examinations and diagnostic tests done by, or at the request of, the attending surgeon will be paid by Medicare, assuming, of course, that the carrier determines the services to be “medically necessary.” All such claims must be accompanied by the appropriate ICD-9 code for preoperative examination ...
What does CPT code 99241 mean?
CPT® Code 99241 - New or Established Patient Office or Other Outpatient Consultation Services - Codify by AAPC. CPT. Evaluation and Management Services. Consultation Services. Office or Other Outpatient Consultation Services.
How long did it take to develop the ICd 10?
Yes, it took almost a decade to create ICD-10, and it has taken more than a decade for the US to actually put the final version of the code set to use. Australia was one of the first countries to adopt ICD-10. Half of the Australian states implemented ICD-10 in 1998, and the rest of the country followed in 1999.
Which countries have adopted the ICD-10 code?
Canada adopted the new code set in 2000, and from there, several European countries as well as Thailand, Korea, China, and South Africa adopted ICD-10 in its original, modified, or translated form. Even Dubai made the switch in 2012.
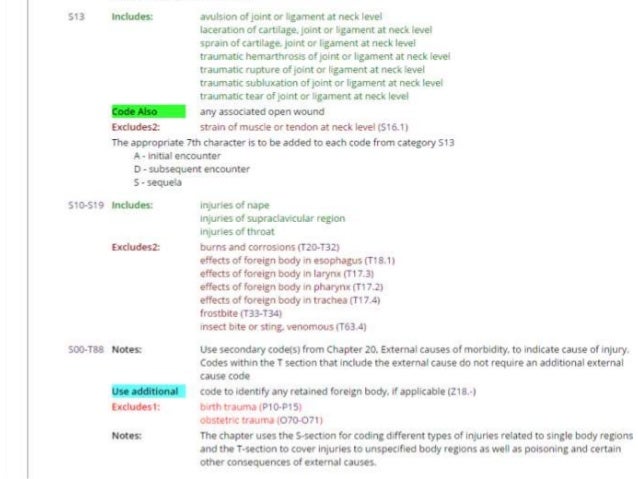
What are external cause codes?
These codes are listed in Chapter 20: External cause codes. They’re secondary codes, which means they expand upon the description of the cause of an injury or health condition by indicating how it happened ( i.e., the cause), the intent ( i.e., intentional or accidental), the location, what the patient was doing at the time of the event, and the patient’s status (e.g., civilian or military). You should use as many external cause codes as necessary to explain the patient’s condition as completely as possible. However, external cause codes need only be used once, usually at the initial encounter.
Is ICd 10 the same as CPT?
Note: ICD-10 codes are completely separate from CPT codes. The transition to ICD-10 does not affect the use of CPT codes. Additionally, ICD-10 codes do not impact guidelines regarding the the KX modifier.
The Patient
The patient is a 16-year-old male high school athlete. During a soccer game last week, his knee came into contact with another player’s leg. He comes directly to physical therapy—without a physician referral—and presents with pain, edema, and instability in his right knee.
The Reason for Outpatient Therapy
Furthermore, you’d want to code the reason the patient is seeking your treatment:
The Description Synonyms
You’ll notice you could code either R26.2 (difficulty walking), or R26.89 (other abnormalities of gait and mobility). That’s because, depending on your evaluation, you might discover the reason behind the disordered movement is best described by one code more than the other. Each code has its own synonyms that can help you make your selection.
The How-To
So, there you have it: An accurate description of an ACL sprain in only eight codes. Easy peasy, right? Want to see how to select ICD-10 codes in WebPT—or how to locate them in the tabular list? Join us for our free ICD-10 bootcamp webinar on August 31. We’ll cover this example—and ones that are even more complex—step-by-step.
When should you use aftercare codes?
If the line between acceptable and unacceptable uses of aftercare codes still seems a bit fuzzy, just remember that in most cases, you should only use aftercare codes if there’s no other way for you to express that a patient is on the “after” side of an aforementioned “before-and-after” event.
What does rehab therapy mean?
The word “rehabilitation” implies restoration. In the rehab therapy space, that usually means restoring health —in other words, getting a patient back to his or her previous, healthy level of musculoskeletal function. So, in many cases, therapists see patients “after” they’ve experienced some type of disruptive event—like an injury, an illness, ...
Why do ICD-10 codes have 7th character?
ICD-10 introduced the seventh character to streamline the way providers denote different encounter types—namely, those in volving active treatment versus those involving subsequent care. However, not all ICD-10 diagnosis codes include the option to add a seventh character. For example, most of the codes contained in chapter 13 of the tabular list (a.k.a. the musculoskeletal chapter) do not allow for seventh characters. And that makes sense considering that most of those codes represent conditions—including bone, joint, or muscle conditions that are recurrent or resulting from a healed injury—for which therapy treatment does progress in the same way it does for acute injuries.
Can you use aftercare codes with injury codes?
Essentially, you are indicating that the patient is receiving aftercare for the injury. Thus, you should not use aftercare codes in conjunction with injury codes, because doing so would be redundant. 3. You can use Z codes to code for surgical aftercare.
Can you use a Z code for aftercare?
In situations where it’s appropriate to use Z codes, “aftercare codes are generally the first listed diagnosis,” Gray writes. However, that doesn’t mean the Z code should be the only diagnosis code listed for that patient.
Do you need a re-evaluation after surgery?
In many cases, yes; a patient who undergoes surgery mid-plan of care should receive a re-evaluation. However, per the above-linked article, "some commercial payers may consider the post-op treatment period a new episode of care, in which case you’d need to use an evaluation code.".
Do therapists use ICD-10 aftercare codes?
Even so, therapists should only use ICD-10 aftercare codes to express patient diagnoses in a very select set of circumstances.
Popular Posts:
- 1. icd 10 code for lsubacute sinusitis
- 2. icd 10 code for ibs
- 3. icd 10 code for medial meniscus tear of the right knee
- 4. billable icd 9 code for deconditioning
- 5. icd 10 code for 27801
- 6. icd 10 pcs code for neurobehavioral and cognitive
- 7. icd 9 code for feeding difficulty
- 8. icd-10 code for restrictive cardiomyopathy
- 9. icd 10 code for lightheadedness dizzy
- 10. icd-10-cm code for cheloid