Lobar pneumonia, unspecified organism
J18. 1 is a billable/specific ICD-10
The International Classification of Diseases (ICD) is a globally used diagnostic tool for epidemiology, health management and clinical purposes. The ICD is maintained by the World Health Organization (WHO), which is the directing and coordinating authority for health within the United Nations System.
https://en.wikipedia.org › wiki › International_Classification_o...
What are the symptoms of left lower lobe pneumonia?
Oct 01, 2021 · Lobar pneumonia, unspecified organism. 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code. J18.1 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM J18.1 became effective on October 1, 2021.
What is right lobe pneumonia?
ICD-10-CM Diagnosis Code C34.31 [convert to ICD-9-CM] Malignant neoplasm of lower lobe, right bronchus or lung. Adenocarcinoma, r lower lobe; Bronchoalveolar carcinoma, r lower lobe; Cancer of the bronchus, right lower lobe; Cancer of the lung, right lower lobe; Large cell carcinoma, r lower lobe; Primary adenocarcinoma of right lower lobe of lung; Primary bronchoalveolar …
What is the ICD 10 code for COPD with pneumonia?
Lobar pneumonia, unspecified organism. 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code. ICD-10-CM Diagnosis Code C34.11 [convert to ICD-9-CM] Malignant neoplasm of upper lobe, right bronchus or lung. Adenocarcinoma, r upper lobe; Bronchoalveolar carcinoma, r upper lobe; Cancer of the bronchus, right upper lobe; Cancer of the lung, right upper lobe; Large cell …
What is the diagnosis code for pneumonia?
Oct 01, 2021 · J16.8 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM J16.8 became effective on October 1, 2021. This is the American ICD-10-CM version of J16.8 - other international versions of ICD-10 J16.8 may differ.

Is lobar pneumonia the same as lower lobe pneumonia?
X-rays play an important role in distinguishing between these types: the term lobar pneumonia is used if an entire lung lobe is visibly inflamed. Depending on which lung lobe is affected, the pneumonia is referred to as upper, middle or lower lobe pneumonia.Aug 9, 2018
How do you code pneumonia in ICD-10?
9.
What is left lower lobe pneumonia?
Lobar pneumonia is a form of pneumonia characterized by inflammatory exudate within the intra-alveolar space resulting in consolidation that affects a large and continuous area of the lobe of a lung.
...
...
| Lobar pneumonia | |
|---|---|
| Specialty | Pulmonology |
What is lobar pneumonia mean?
It is a serious infection in which the air sacs fill with pus and other liquid. Lobar pneumonia affects one or more sections (lobes) of the lungs. Bronchial pneumonia (also known as bronchopneumonia) affects patches throughout both lungs.
What is the diagnosis for ICD-10 code r50 9?
9: Fever, unspecified.
Is pneumonia a lower respiratory infection?
Pneumonia as the Most Common Lower Respiratory Tract Infection.
What is the ICD 10 code for left lower lobe pneumonia?
Lobar pneumonia, unspecified organism
J18. 1 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM J18. 1 became effective on October 1, 2021.
J18. 1 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM J18. 1 became effective on October 1, 2021.
What causes lower lobe pneumonia?
Most cases of lobar pneumonia are community acquired and caused by Streptococcus pneumoniae. Other causes include Klebsiella pneumoniae, Legionella pneumophila, Haemophilus influenzae, and Mycobacterium tuberculosis.
Does lower lobe infiltrate mean pneumonia?

Answer. Radiographic evidence of aspiration pneumonia depends on the position of the patient when the aspiration occurred. The right lower lung lobe is the most common site of infiltrate formation due to the larger caliber and more vertical orientation of the right mainstem bronchus.Aug 15, 2018
How many lobes does the right lung have?
3 lobes
Each lung is divided into lobes (sections): The right lung has 3 lobes and is slightly larger than the left lung. The left lung has 2 lobes. The heart sits in the cardiac notch, which is a groove in the lower lobe.
What are the 4 different types of pneumonia?
These are:
- Bacterial pneumonia. This is caused by bacteria, the most common of which is streptococcus pneumoniae. ...
- Viral pneumonia. Responsible for about one-third of all pneumonia cases, this type is caused by various viruses, includingflu (influenza). ...
- Mycoplasma pneumonia. ...
- Fungal pneumonia.
What are the 5 types of pneumonia?
Articles On Pneumonia Types
- Types of Pneumonia.
- Walking Pneumonia.
- Viral Pneumonia.
- Bacterial Pneumonia.
- Chemical Pneumonia.
Apr 8, 2020
What causes lobar pneumonia?
The most common cause for this type of pneumonia is Streptococcus pneumoniae (pneumococcus). Other common types of bacteria responsible for “lobar” pneumonia are: 1 Klebsiella pneumoniae 2 Legionella pneumophila 3 Haemophilus influenza 4 Mycobacterium tuberculosis
What is non-segmental pneumonia?
The antibiotic will be chosen based on the causative organism identified or suspected. This type of pneumonia is also referred to as “non-segmental” or “focal non-segmental” pneumonia and is often referred to in CT of the chest to have the appearance of “ground glass opacity.”.
How many stages of pneumonia are there?
This type of pneumonia is typically acute with four stages:
What are the common clinical complications of pneumonia?
Complications can include pleural/parapneumonic effusion and empyema.
Can lobar pneumonia be coded?
This is different than having the presence of an infiltrate in the lobe of the lung. Lobar pneumonia should only be coded when the physician/provider specifically documents “lobar pneumonia” and there is no causal organism specified.
What are the different types of pneumonia?
Common types of pneumonia include community-acquired pneumonia (CAP), healthcare-associated (HCAP), hospital-acquired (HAP), and aspiration pneumonia (AP).
How severe is bronchopneumonia?
The severity of bronchopneumonia can range from mild to severe, and the prognosis is basically determined according to the severity of the underlying disease.
What is the name of the inflammation of the small airways in the lungs?
Bronchopneumonia, also referred to as bronchial pneumonia, multifocal, or lobular pneumonia, is an acute inflammation of the small airways within the lungs (bronchioles) and the surrounding lung tissue (alveoli). The cause of bronchopneumonia, like lobar pneumonia, is usually bacterial.
What is the infection that affects the air sacs in one or both lungs?
Pneumonia is a common infection that affects the air sacs in one or both lungs. Unfortunately, when the air sacs fill with pus and other liquid, the infection can become quite serious and even fatal.
What are the risk factors for bronchopneumonia?
Risk factors for this condition include infants and young children, people over 65, smoking, being bedridden, and underlying conditions such as flu, measles, cystic fibrosis, and chronic bronchitis. Diagnosing bronchopneumonia includes a blood test and sputum culture to determine the causative microbe.
Is pneumonia fatal?
Conclusion. Pneumonia is a serious and potentially fatal condition. Therefore, the coder must assign the specific ICD-10 code that reflects the severity, acuity and risk of mortality. In addition, the coder must understand the different types of pneumonia, such as lobar pneumonia and bronchopneumonia.
Is bronchopneumonia a bacterial infection?
The cause of bronchopneumonia, like lobar pneumonia, is usually bacterial. The bacteria may be Staphylococcus aureus, Klebsiella pneumoniae, Haemophilus influenzae, Pseudomonas aeruginosa, or Escherichia coli. Bronchopneumonia usually occurs in hospital patients (hospital-acquired) and patients requiring a breathing machine. It also occurs in a person who aspirates vomit and in intravenous drug abusers. Other causes of bronchopneumonia include atypical bacterium Mycoplasma, fungi, and viruses.
What is the ICD code for lobar pneumonia?
J18.1 is a billable ICD code used to specify a diagnosis of lobar pneumonia, unspecified organism. A 'billable code' is detailed enough to be used to specify a medical diagnosis.
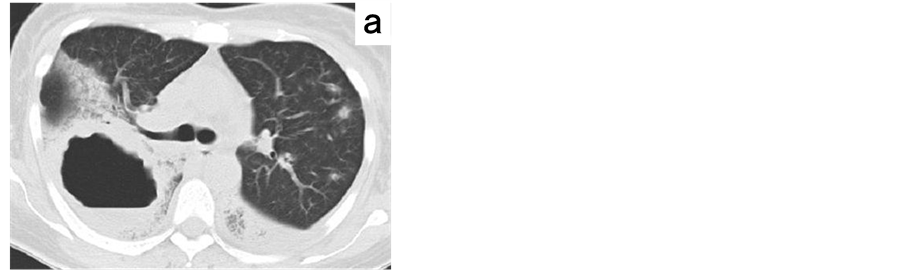
What is the figure A in the lung?
Figure A shows the location of the lungs and airways in the body. This figure also shows pneumonia affecting the lower lobe of the left lung. Figure B shows normal alveoli. Figure C shows infected alveoli.
What is DRG group #193-195?
DRG Group #193-195 - Simple pneumonia and pleurisy with CC.
What is the diagnosis of lobar pneumonia?
A diagnosis of "lobar pneumonia" (pneumonia that mentions the affected lobe) or "multilobar pneumonia" (pneumonia affecting more than one lobe) describes the specific site of the pneumonia (rather than a type of pneumonia) and would be coded according to the responsible organism, if known.
What is the code for pneumonitis due to fumes and vapors?
pneumonitis due to fumes and vapors (J68.0) usual interstitial pneumonia (J84.17) Guidelines: Diseases of the respiratory system (J00-J99) Use additional code, where applicable, to identify:exposure to environmental tobacco smoke (Z77.22)
What is 481 in a strep?
481 is J13 pneumonia due to Strep and J18.1 Lobar pneumonia, unspecified organism. How would you code "Left Lower lobe pneumonia" please site reasons and preferably documentation of guideline.
When a respiratory condition is described as occurring in more than one site and is not specifically indexed, it should be
Note: When a respiratory condition is described as occurring in more than one site and is not specifically indexed, it should be classified to the lower anatomic site (e.g. tracheobronchitis to bronchitis in J40).
Is 486 a diagnosis of pneumonia?
No. The diagnosis of right lower lobe pneumonia without further specification as to type of pneumonia or the specific organism involved is coded 486. The entry in the first printing of the Alphabetic Index for Pneumonia, lobe-see Pneumonia, lobar - should be deleted from the Alphabetic Index. lobar pneumonia is a synonym (interchangeable term) for pneumococcal pneumonia, 481.
Popular Posts:
- 1. icd-10 code for perirectal abscess
- 2. icd 1 code for asthma in pregnancy
- 3. icd 10 code for direct blow
- 4. icd 10 code for aftercare following sigmoid colectomy
- 5. 2018 icd 10 code for phlebitis
- 6. icd 10 code for acute inferior wall myocardial infarction
- 7. icd 9 code for suprapubic pain
- 8. icd 10 cm code for bipolar manic depressive
- 9. icd 10 code for vit ana
- 10. icd 10 code for gait dysfunction