S43.432A
What is the ICD 10 code for left posterior labral tear?
S43.432AICD-10-CM Code for Superior glenoid labrum lesion of left shoulder, initial encounter S43. 432A.
What is the ICD 10 code for posterior labral tear?
The ICD-10-CM code S43. 432A might also be used to specify conditions or terms like anterior to posterior tear of superior glenoid labrum of left shoulder or glenoid labrum tear.
What is the ICD 10 code for right shoulder posterior labral tear?
S43.431AICD-10-CM Code for Superior glenoid labrum lesion of right shoulder, initial encounter S43. 431A.
What is a posterior labral tear?
Posterior Labral Tear (Lesion) This is a condition of the shoulder which usually affects younger people. It is most commonly caused by a fall onto the arm or a direct blow e.g. a rugby tackle. It is also seen in people who do a lot of throwing. The glenoid has a rim of tissue (the labrum) around its edge.
What is the ICD-10 code for left shoulder pain?
ICD-10 | Pain in left shoulder (M25. 512)
What is the ICD-10 code for left shoulder bursitis?
ICD-10 | Bursitis of left shoulder (M75. 52)
What is the ICD-10 code for left shoulder synovitis?
M65.812ICD-10 | Other synovitis and tenosynovitis, left shoulder (M65. 812)
What is ICD-10 code for left shoulder instability?
M25.312ICD-10 | Other instability, left shoulder (M25. 312)
What is ICD-10 code for rotator cuff tear?
A traumatic rotator cuff diagnosis is defined as an injury of the rotator cuff ligaments, muscles, and tendons and maps to rotator cuff sprain/strain and/or tear/rupture. ICD-10 codes S46. 011A (right shoulder) and S46. 012A (left shoulder) are for strain/tear/rupture OR S43.
What is a labral tear in the shoulder?
The labrum is a piece of fibrocartilage (rubbery tissue) attached to the rim of the shoulder socket that helps keep the ball of the joint in place. When this cartilage is torn, it is called a labral tear. Labral tears may result from injury, or sometimes as part of the aging process.
Where is the posterior labrum?
The labrum is a type of cartilage found in the shoulder joint. The shoulder is a ball-and-socket joint where the arm meets the body.
What causes a posterior labral tear?
Causes and risk factors Traumatic injury and wear and tear from repetitive motion of the upper arm can both cause labrum tears. Some specific causes of labrum tears include: a fall on an outstretched arm. a direct hit to the shoulder.
What is posterior shoulder instability?
Posterior shoulder instability may result in injury to the posterior band of the inferior glenohumeral ligament as well as the posterior labrum, or a reverse Bankart lesion. Tears can extend to involve multiple regions of the labrum and have other associated injuries.
What causes a slap tear in the shoulder?
The most common mechanisms for SLAP tears are forced traction on the shoulder and direct compression. Direct compression can occur in the acute traumatic setting or in the chronic setting typical in the overhead throwing athlete. Overhead throwers are predisposed to SLAP tears secondary to their adaptive anatomy.
What is the labrum?
The labrum also serves as an attachment point for the long head of the biceps tendon, the glenohumeral ligaments, and the long head of the triceps tendon, forming a periarticular system of fibers that gives the shoulder joint much needed stability [ 4 ]. The vascular supply to the labrum is from the posterior humeral circumflex artery, ...
How to tell if a slap tear is a slap?
A patient with a SLAP tear will most commonly present with symptoms of deep-seated pain, which can be sharp or dull [ 11 ]. It is usually located deep within the center of the shoulder and can be made worse with overhead activities, pushing heavy objects, lifting, or reaching behind the back. Patients may have mechanical symptoms, such as catching, popping, or grinding with rotation of the shoulder. Many patients with a SLAP tear will also have other shoulder disease, making clinical diagnosis challenging [ 11 ].
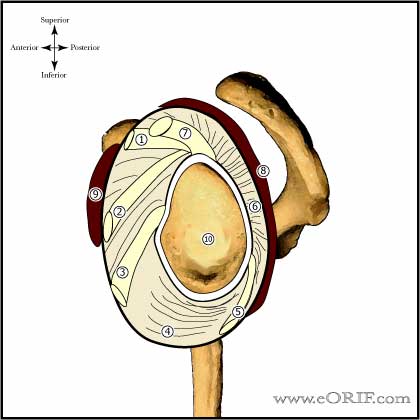
Where do bicep tendon tears occur?
Approximately 40% to 60% of the biceps tendon originates from the supraglenoid tubercle, and the remaining fibers insert into the labrum [ 1 ]. The biceps insertion into the labrum is variable but most commonly is in a more posterior position. FIGURE 15.1 Normal anatomy of the shoulder. Tears can occur in all regions of the labrum.
What is SLAP tear?
The most studied injury to the labrum is the superior labral anterior-posterior (SLAP) tear. Anterior dislocations of the shoulder can be associated with a disruption of the anteroinferior labrum and anterior band of the inferior glenohumeral ligament, also known as a Bankart lesion.
What are the symptoms of a slap tear?
Patients may have mechanical symptoms, such as catching, popping, or grinding with rotation of the shoulder. Many patients with a SLAP tear will also have other shoulder disease, making clinical diagnosis challenging [ 11 ].
What is the ICd 10 code for glenoid labrum?
S43.432A is a billable diagnosis code used to specify a medical diagnosis of superior glenoid labrum lesion of left shoulder, initial encounter. The code S43.432A is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.#N#The ICD-10-CM code S43.432A might also be used to specify conditions or terms like anterior to posterior tear of superior glenoid labrum of left shoulder or glenoid labrum tear.#N#S43.432A is an initial encounter code, includes a 7th character and should be used while the patient is receiving active treatment for a condition like superior glenoid labrum lesion of left shoulder. According to ICD-10-CM Guidelines an "initial encounter" doesn't necessarily means "initial visit". The 7th character should be used when the patient is undergoing active treatment regardless if new or different providers saw the patient over the course of a treatment. The appropriate 7th character codes should also be used even if the patient delayed seeking treatment for a condition.
How to diagnose shoulder pain?
Health care providers diagnose shoulder problems by using your medical history, a physical exam, and imaging tests. Often, the first treatment for shoulder problems is RICE. This stands for Rest, Ice, Compression, and Elevation. Other treatments include exercise and medicines to reduce pain and swelling.
What are the bones of the shoulder?
Your shoulder joint is composed of three bones: the clavicle (collarbone), the scapula (shoulder blade), and the humerus (upper arm bone). Your shoulders are the most movable joints in your body. They can also be unstable because the ball of the upper arm is larger than the shoulder socket that holds it.
How to tell if you have a sprain or strain?
At first, treatment of both sprains and strains usually involves resting the injured area, icing it, wearing a bandage or device that compresses the area, and medicines. Later treatment might include exercise and physical therapy.
What is the GEM crosswalk?
The General Equivalency Mapping (GEM) crosswalk indicates an approximate mapping between the ICD-10 code S43.432A its ICD-9 equivalent. The approximate mapping means there is not an exact match between the ICD-10 code and the ICD-9 code and the mapped code is not a precise representation of the original code.
What is the labrum of the shoulder?
The glenoid labrum is a densely fibrous tissue that is located along the periphery of the glenoid portion of the scapula. It functions to provide increased stability, while still allowing great range of motion. In addition, it serves as an attachment point for tendons and ligaments. Tears can occur in all regions of the labrum. The two most common sites include the superior labral anterior-posterior (SLAP) tear, occurring with forced traction of the shoulder and/or direct compression, and the Bankart lesion, created by episodes of anterior instability. Symptoms of deep-seated pain (SLAP tears) or anterior instability (Bankart lesions) are the most common presentations, but concomitant shoulder pathology makes diagnosis challenging and clouds many physical exam findings. Physical exam includes several clinical tests, with the O’Brien’s test being the most common for SLAP tears and the surprise test as the most accurate for Bankart lesions. As in any case of shoulder pain, the initial imaging of choice is plain radiography. With a high clinical likelihood of labral disease, this should be followed by either magnetic resonance imaging or magnetic resonance arthrography. Initial management of SLAP tears involves exhausting non-operative treatment, focusing on stretching and strengthening of the dynamic shoulder stabilizers. Initial management of Bankart lesions (after reduction) may be conservative or operative and depends on demographic and radiographic factors. Surgical management of SLAP tears are reserved for those who have failed conservative management. Operative treatment of Bankart tears are reserved for those with recurrent instability despite conservative treatment.
What is posterior shoulder instability?
Posterior shoulder instability may result in injury to the posterior band of the inferior glenohumeral ligament as well as the posterior labrum, or a reverse Bankart lesion. Tears can extend to involve multiple regions of the labrum and have other associated injuries.
How to tell if a slap tear is a slap?
A patient with a SLAP tear will most commonly present with symptoms of deep-seated pain, which can be sharp or dull. It is usually located deep within the center of the shoulder and can be made worse with overhead activities, pushing heavy objects, lifting, or reaching behind the back. Patients may have mechanical symptoms, such as catching, popping, or grinding with rotation of the shoulder. One study found that in 139 patients demonstrating a SLAP lesion on shoulder arthroscopy, 123 patients (88%) also had other intra-articular lesions, making clinical diagnosis challenging.
Where do biceps tendons come from?
Approximately 40% to 60% of biceps tendons originate from the supraglenoid tubercle, and the remaining fibers insert into the labrum. The biceps insertion into the labrum is variable, but most commonly is in a more posterior position. Normal anatomy of the shoulder. Tears can occur in all regions of the labrum.
What imaging is used for shoulder pain?
As in any case of shoulder pain, the initial imaging of choice is plain radiography. With a high clinical likelihood of labral disease, this should be followed by either magnetic resonance imaging or magnetic resonance arthrography.
What is the labrum?
The labrum also serves as an attachment point for the long head of the biceps tendon, the glenohumeral ligaments, and the long head of the triceps tendon, forming a periarticular system of fibers that gives the shoulder joint much needed stability .
What is SLAP tear?
The most studied injury to the labrum is the superior labral anterior-posterior (SLAP) tear. Anterior dislocations of the shoulder can be associated with a disruption of the anteroinferior labrum and anterior band of the inferior glenohumeral ligament, also known as a Bankart lesion.
What is the ICd 10 code for glenoid labrum tear?
S43.432D is a billable diagnosis code used to specify a medical diagnosis of superior glenoid labrum lesion of left shoulder, subsequent encounter. The code S43.432D is valid during the fiscal year 2021 from October 01, 2020 through September 30, 2021 for the submission of HIPAA-covered transactions.#N#The ICD-10-CM code S43.432D might also be used to specify conditions or terms like anterior to posterior tear of superior glenoid labrum of left shoulder or glenoid labrum tear. The code is exempt from present on admission (POA) reporting for inpatient admissions to general acute care hospitals.#N#S43.432D is a subsequent encounter code, includes a 7th character and should be used after the patient has completed active treatment for a condition like superior glenoid labrum lesion of left shoulder. According to ICD-10-CM Guidelines a "subsequent encounter" occurs when the patient is receiving routine care for the condition during the healing or recovery phase of treatment. Subsequent diagnosis codes are appropriate during the recovery phase, no matter how many times the patient has seen the provider for this condition. If the provider needs to adjust the patient's care plan due to a setback or other complication, the encounter becomes active again.
How to diagnose shoulder pain?
Health care providers diagnose shoulder problems by using your medical history, a physical exam, and imaging tests. Often, the first treatment for shoulder problems is RICE. This stands for Rest, Ice, Compression, and Elevation. Other treatments include exercise and medicines to reduce pain and swelling.
What is the GEM crosswalk?
The General Equivalency Mapping (GEM) crosswalk indicates an approximate mapping between the ICD-10 code S43.432D its ICD-9 equivalent. The approximate mapping means there is not an exact match between the ICD-10 code and the ICD-9 code and the mapped code is not a precise representation of the original code.
What are the bones of the shoulder?
Your shoulder joint is composed of three bones: the clavicle (collarbone), the scapula (shoulder blade), and the humerus (upper arm bone). Your shoulders are the most movable joints in your body. They can also be unstable because the ball of the upper arm is larger than the shoulder socket that holds it.
Is S43.432D a POA?
S43.432D is exempt from POA reporting - The Present on Admission (POA) indicator is used for diagnosis codes included in claims involving inpatient admissions to general acute care hospitals. POA indicators must be reported to CMS on each claim to facilitate the grouping of diagnoses codes into the proper Diagnostic Related Groups (DRG). CMS publishes a listing of specific diagnosis codes that are exempt from the POA reporting requirement. Review other POA exempt codes here.
Popular Posts:
- 1. icd 10 code for right left thigh swelling
- 2. icd 10 code for a fiv
- 3. what is the icd-10-cm code for prostate hyperplasia with urinary retention?
- 4. icd 10 code for diminished blood flow to lower extremity
- 5. icd-10 code for atypical nevus
- 6. icd-10 code for developmental delay in adults
- 7. icd 10 code for testicular microlithiasis
- 8. what is the correct icd 10 code for organophosphate toxicity
- 9. icd 10 cm code for latent tb
- 10. icd 10 code for pxe ophthalmology