ICD-10 Code for Abnormal results of pulmonary function studies- R94. 2- Codify by AAPC.
What is Procedure Code 10e0xzz?
Section C - The following ICD-10-CM codes are covered for CPT codes 94013, 94450, 94617, 94618, 94619, 94621, 94640, 94664, 94680, 94681, 94690, 94726, 94727, 94728 and 94729. For the utilization of CPT code 94664, see the Pulmonary Function Testing codes in the Article Text section above. Group 3 Codes
How is pulmonary function testing used for COPD?
Abnormal lung function testing; Lung function testing abnormal; Reduced ventilatory capacity; Reduced vital capacity ICD-10-CM Diagnosis Code R94.2 …
What is the ICD 10 diagnosis code for?
Oct 01, 2021 · Z13.83 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z13.83 became effective on October 1, 2021. This is the American ICD-10-CM version of Z13.83 - other international versions of ICD-10 Z13.83 may differ. Type 1 Excludes.
What is diagnosis code 10?
Oct 01, 2021 · Abnormal results of pulmonary function studies. 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code. R94.2 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM R94.2 became effective on October 1, 2021.

What is the CPT code for pulmonary function test?
Billing For Pulmonary Procedures
| Procedure | CPT Code |
|---|---|
| Pulmonary Function Testing—no bronchodilator | 94010 |
| Pulmonary Function Testing pre and post bronchodilator | 94060 |
| Aerosol treatment (includes demonstration)* | 94640 |
| Demonstration | 94664 |
What is the ICD-10 code for pulmonary?
4: Other disorders of lung.
What is the CPT code for pulmonary stress test?
CPT code 94618 Pulmonary stress testing (eg, 6-minute walk test), including measurement of heart rate, oximetry, and oxygen titration, when performed describes the typical simple pulmonary stress test.Jan 1, 2018
What is a full pulmonary function test?
Pulmonary function tests (PFTs) are noninvasive tests that show how well the lungs are working. The tests measure lung volume, capacity, rates of flow, and gas exchange. This information can help your healthcare provider diagnose and decide the treatment of certain lung disorders.
What is DX code J98 4?
J98. 4 - Other disorders of lung. ICD-10-CM.
What is diagnosis code R91 8?
Other nonspecific abnormal finding of lung field
ICD-10 code R91. 8 for Other nonspecific abnormal finding of lung field is a medical classification as listed by WHO under the range - Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
Is a pulmonary function test covered by Medicare?
The various modalities to assess pulmonary function must be used in a purposeful and logical sequence. Tests performed as components rather than as a single test will be denied. Medicare does not cover screening tests.
What does CPT code 94761 mean?
94761, noninvasive ear or pulse oximetry for oxy- gen saturation; multiple determinations (eg, during exercise). Multiple pulse oximetry with several Sao2 (Spo2) determinations reported usually taken while the patient is sitting, standing, and walking.
What does CPT code 93017 mean?
Cardiovascular stress test
CPT® Code 93017 in section: Cardiovascular stress test using maximal or submaximal treadmill or bicycle exercise, continuous electrocardiographic monitoring, and/or pharmacological stress.
What are pulmonary function tests and what are two examples?
If you are having trouble breathing, or some type of chronic respiratory illness, your doctor might order pulmonary function tests to find out how well your lungs are working. These might include spirometry, lung volume testing, and a six-minute walk test.Sep 27, 2018
What are the different pulmonary function tests?
They include:
- Spirometry. the most common type of lung function test. ...
- Lung volume test. also known as body plethysmography. ...
- Gas diffusion test. This test measures how oxygen and other gases move from the lungs to the bloodstream.
- Exercise stress test. This test looks at how exercise affects lung function.
Sep 9, 2021
Who does pulmonary function test?
Pulmonary function test results
A pulmonologist is a doctor who specializes in lung health. They'll review and interpret your tests and send the results to your doctor. You may have to wait 48 to 72 hours to get those results and discuss them with your doctor.
A pulmonologist is a doctor who specializes in lung health. They'll review and interpret your tests and send the results to your doctor. You may have to wait 48 to 72 hours to get those results and discuss them with your doctor.
What is the ICd 10 code for respiratory disease?
Encounter for screening for respiratory disorder NEC 1 Z13.83 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. 2 The 2021 edition of ICD-10-CM Z13.83 became effective on October 1, 2020. 3 This is the American ICD-10-CM version of Z13.83 - other international versions of ICD-10 Z13.83 may differ.
When will the ICD-10 Z13.83 be released?
The 2022 edition of ICD-10-CM Z13.83 became effective on October 1, 2021.
What is screening for asymptomatic individuals?
Screening is the testing for disease or disease precursors in asymptomatic individuals so that early detection and treatment can be provided for those who test positive for the disease. Type 1 Excludes. encounter for diagnostic examination-code to sign or symptom. Encounter for screening for other diseases and disorders.
How often do you need to treat ICd 10 codes?
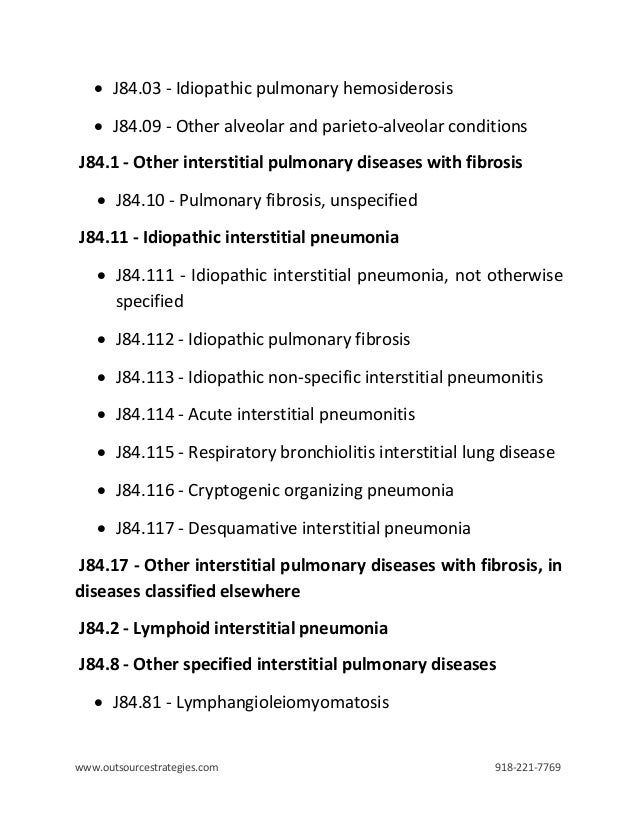
Treatment for the following ICD-10 codes may require treatments up to four times per year: J84.10, J84.170, J84.178, J84.89 or J84.112. Refer to the related LCD for information regarding services for these diagnoses.
Why do contractors need to specify revenue codes?
Contractors may specify Revenue Codes to help providers identify those Revenue Codes typically used to report this service. In most instances Revenue Codes are purely advisory. Unless specified in the article, services reported under other Revenue Codes are equally subject to this coverage determination. Complete absence of all Revenue Codes indicates that coverage is not influenced by Revenue Code and the article should be assumed to apply equally to all Revenue Codes.
Can you bill CPT/HCPCS with all billing codes?
Note: The contractor has identified the Bill Type and Revenue Codes applicable for use with the CPT/HCPCS codes included in this article. Providers are reminded that not all CPT/HCPCS codes listed can be billed with all Bill Type and/or Revenue Codes listed. CPT/HCPCS codes are required to be billed with specific Bill Type and Revenue Codes. Providers are encouraged to refer to the CMS Internet-Only Manual (IOM) Publication 100-04, Medicare Claims Processing Manual, for further guidance.
Is CPT a year 2000?
CPT is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to, the implied warranties of merchantability and fitness for a particular purpose. AMA warrants that due to the nature of CPT, it does not manipulate or process dates, therefore there is no Year 2000 issue with CPT. AMA disclaims responsibility for any errors in CPT that may arise as a result of CPT being used in conjunction with any software and/or hardware system that is not Year 2000 compliant. No fee schedules, basic unit, relative values or related listings are included in CPT. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this file/product is with CMS and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this file/product. This Agreement will terminate upon no upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
What tests can detect lung dysfunction?
Detect the presence or absence of lung dysfunction suggested by other abnormal diagnostic tests (e.g., radiography, arterial blood gas analysis).
What is pulmonary stress test?
The simple pulmonary stress testing is a test that allows quantification of workload and heart rate activity, while measuring the degree of oxygen desaturation. This test is undertaken to measure the degree of hypoxemia or desaturation that occurs with exertion. It is also used to optimize titration of supplemental oxygen for the correction of hypoxemia.
What is post bronchodilator spirometry?
Post-bronchodilator spirometry is used to evaluate the reversible component of bronchospasm and to determine if the patient is a bronchodilator therapy candidate. Claims for spirometry will be subject to medical review as follows: there are clinical signs and symptoms consistent with bronchospasm; or spirometry without bronchodilator is abnormal; or reversibility or nonreversibility of bronchospasm has not been demonstrated. Repeat studies are covered only with clinically significant change, necessitating adjustment/augmentation of therapy, appropriately documented.
Is spirometry contraindicated for thoracic surgery?
General clinical contraindications to spirometry include: hemoptysis of unknown origin, pneumothorax, unstable cardiovascular status, thoracic/abdominal or cerebral aneurysms, recent eye surgery, recent thoracic or abdominal surgery, and presence of acute disease processes that interfere with test performance.
Does Medicare cover lung screening?
Medicare does not cover screening tests. Medicare coverage excludes routine (screening) tests for asymptomatic patients with or without high risk of lung disease (e.g., prolonged smoking history). It also excludes studies as part of a routine exam, and studies as part of an epidemiological survey.
Is CPT a year 2000?
CPT is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to, the implied warranties of merchantability and fitness for a particular purpose. AMA warrants that due to the nature of CPT, it does not manipulate or process dates, therefore there is no Year 2000 issue with CPT. AMA disclaims responsibility for any errors in CPT that may arise as a result of CPT being used in conjunction with any software and/or hardware system that is not Year 2000 compliant. No fee schedules, basic unit, relative values or related listings are included in CPT. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this file/product is with CMS and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this file/product. This Agreement will terminate upon no upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
What is the most commonly used section of Pulmonary Function Testing?
Spirometry makes up the most commonly applied section of Pulmonary Function Testing (PFT). General indications are:
What is the evaluation of lung function?
The evaluation of lung function is indicated to determine: The presence of lung disease or abnormality of lung function. The extent of abnormalities and the potential causative disease process. The extent of disability due to abnormal lung function. The progression of the disease.
What is post bronchodilator spirometry?
Limitations: Post-bronchodilator spirometry is used to rule out a reversible component to a patient’s bronchospasm and determine if the patient is a candidate for bronchodilator therapy.
What is DLCO in pulmonary spirometry?
Diffusion capacity (DLCO) measurement is often indicated when spirometry and lung volume studies reveal restrictive disease. DLCO is used to help distinguish between an intrinsic pulmonary process, such as interstitial lung disease and emphysema, and an extrapulmonary process, such as chest wall and neuromuscular disorders. Diffusion capacity is also useful in quantifying the degree of parenchymal destruction in COPD, and assessing pulmonary vascular diseases and interstitial diseases, even if vital capacity is normal.
How many attempts are required for spirometry?
Spirometry studies, in particular, require a minimum of three attempts that must meet minimum acceptability criteria.
Why is lung compliance more invasive than other PFTs?
It is more invasive than other PFTs, because the patient is required to swallow an esophageal balloon. Compliance studies are performed only when all other PFTs give equivocal results or the results require confirmation by additional data. Lung compliance may be increased in emphysema and reduced in interstitial lung disease.
When will bronchodilator study (94060) be covered?
If reversibility of bronchospasm (bronchodilator responsiveness) has already been either ruled out or demonstrated, repeat pre- and post-bronchodilator study (94060) will be covered only when there is a significant clinical change in the patient’s functional respiratory status necessitating an adjustment or augmentation of bronchoactive medications, and this is documented in the patient’s medical record.
Popular Posts:
- 1. icd code for diabetes type 2 due to steroid usage
- 2. what is a icd 10 code for acute recurrent maxillary sinusitis
- 3. icd 10 cm code for femynor
- 4. 2015 icd 10 code for cholelithiasis
- 5. icd 10 code for asymmetric hemiatrophy
- 6. icd 10 cm code for hyperkalemia
- 7. icd 10 code for unspeciied accident
- 8. icd 10 code for personal history of knee replacement
- 9. icd 10 code for lung abnormality
- 10. icd 10 code for inhaler refill.