Z96. 651 - Presence of right artificial knee joint. ICD-10-CM.
Full
AnswerWhat is the ICD 10 code for total knee replacement?
27487 Revision of total knee arthroplasty, with or without allograft; femoral and entire tibial component Removal 27488 Removal of prosthesis, including total knee prosthesis, methylmethacrylate with or without insertion of spacer, knee Hospital Inpatient: ICD-10-PCS Code and Description
What is the ICD 10 code for presence of right artificial knee?
Presence of right artificial knee joint. Z96.651 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2019 edition of ICD-10-CM Z96.651 became effective on October 1, 2018.
What is the ICD 10 code for Felty's syndrome of right knee?
Post-immunization arthropathy of right knee; Postimmunization arthropathy of right knee ICD-10-CM Diagnosis Code M05.061 [convert to ICD-9-CM] Felty's syndrome, right knee Felty's syndrome of right knee; Feltys syndrome of bilateral knees; Feltys syndrome of right knee
What is the CPT code for knee arthroplasty?
Knee Systems Coding Reference Guide Physician CPT®Code Description Arthroplasty 27440Arthroplasty, knee, tibial plateau 27441Arthroplasty, knee, tibial plateau; with debridement and partial synovectomy 27442Arthroplasty, femoral condyles or tibial plateau(s), knee
How do you code a total knee replacement?
This procedure would be reported using code 27447-58, 22—Arthroplasty, knee, condyle and plateau; medial AND lateral compartments with or without patella resurfacing (total knee arthroplasty).
What is the ICD code for knee replacement?
ICD-10: Z96. 651, Status (post), organ replacement, by artificial or mechanical device or prosthesis of, joint, knee-see presence of knee joint implant.
What is the ICD-10-CM code for knee surgery?
Presence of right artificial knee joint The 2022 edition of ICD-10-CM Z96. 651 became effective on October 1, 2021.
What is the ICD 10 code for status post left total knee arthroplasty?
652.
What is the ICD-10 code for history of knee surgery?
653.
Can Z47 1 be a primary diagnosis code?
For example, if a patient with severe degenerative osteoarthritis of the hip, underwent hip replacement and the current encounter/admission is for rehabilitation, report code Z47. 1, Aftercare following joint replacement surgery, as the first-listed or principal diagnosis.
What is a right total knee arthroplasty?
Knee replacement, also called knee arthroplasty or total knee replacement, is a surgical procedure to resurface a knee damaged by arthritis. Metal and plastic parts are used to cap the ends of the bones that form the knee joint, along with the kneecap.
What is the ICD-10 code for aftercare following joint replacement?
ICD-10 code Z47. 1 for Aftercare following joint replacement surgery is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is the ICD-10 code for status post surgery?
ICD-10-CM Code for Encounter for surgical aftercare following surgery on specified body systems Z48. 81.
When do you use Z47 2?
ICD-10 code Z47. 2 for Encounter for removal of internal fixation device is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
When do you use Z09?
This second example uses Z09, which indicates surveillance following completed treatment of a disease, condition, or injury. Its use implies that the condition has been fully treated and no longer exists. Z09 would be used for all annual follow-up exams, provided no complications or symptoms are present.
When should aftercare codes be used?
Aftercare visit codes are assigned in situations in which the initial treatment of a disease has been performed but the patient requires continued care during the healing or recovery phase, or for the long-term consequences of the disease.
What is the ICD 10 code for knee pain?
ICD-10 Code for Pain in unspecified knee- M25. 569- Codify by AAPC.
What is the ICD 10 code for bilateral TKA?
Z96. 653 - Presence of artificial knee joint, bilateral. ICD-10-CM.
What is the ICD 10 code for pain in left knee?
562 Pain in left knee.
What is the ICD 10 code for osteoarthritis of left knee?
ICD-10-CM Code for Unilateral primary osteoarthritis, left knee M17. 12.
When will the ICD-10 Z96.651 be released?
The 2022 edition of ICD-10-CM Z96.651 became effective on October 1, 2021.
What is a Z77-Z99?
Z77-Z99 Persons with potential health hazards related to family and personal history and certain conditions influencing health status
What is the procedure code for knee replacement?
The procedure code 0SRC0L9 is in the medical and surgical section and is part of the lower joints body system, classified under the replacement operation. The applicable bodypart is knee joint, right.
What is the code for replacement of knee joint?
0SRC0L9 is a billable procedure code used to specify the performance of replacement of right knee joint with medial unicondylar synthetic substitute, cemented, open approach. The code is valid for the year 2021 for the submission of HIPAA-covered transactions.
What is ICD-10-PCS?
The ICD-10 Procedure Coding System (ICD-10-PCS) is a catalog of procedural codes used by medical professionals for hospital inpatient healthcare settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates. These 2022 ICD-10-PCS codes are to be used for discharges occurring from October 1, 2021 through September 30, 2022.
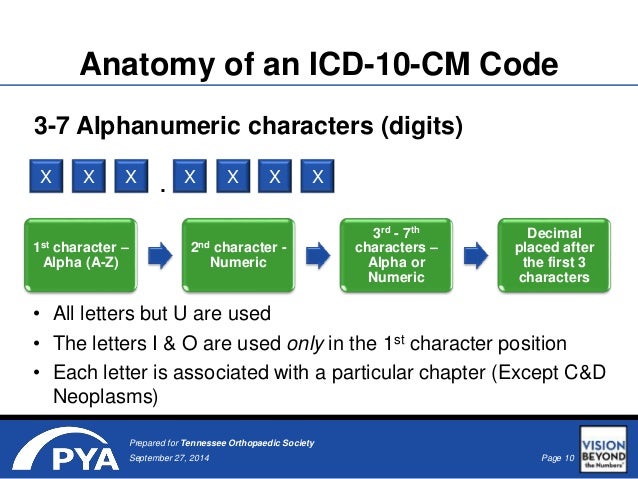
How many decimals are in the ICD-10 code?
Each ICD-10-PCS code has a structure of seven alphanumeric characters and contains no decimals . The first character defines the major "section". Depending on the "section" the second through seventh characters mean different things.
What is removal procedure?
A Removal procedure is coded for taking out the device used in a previous replacement procedure. The body part may have been taken out or replaced, or may be taken out, physically eradicated, or rendered nonfunctional during the Replacement procedure.
What is total knee replacement?
Next, let’s take a look at a practical application. Consider a total knee replacement, which consists of the replacing of all three components of the knee joint (the tibial, femoral, and patellar components). The first time the total joint is replaced with an orthopedic device, the procedure would be coded to replacement based on the definition of the ICD-10-PCS root operation of the same name. The removal of the native joint would not be coded separately because it is considered to be inherent to the process to replace the joint.
What is replacement in medical terminology?
Replacement: putting in or on biological or synthetic material that physically takes the place and/or function of all or a portion of a body part. Removal: taking out or off a device from a body part. Revision: Correcting to the extent possible a portion of a malfunctioning device or the position of a displaced device.
What is removal procedure?
A removal procedure is coded for taking out a device that was used in a previous replacement procedure; in other words, a complete re-do. If the previously placed device is completely removed and replaced, both removal and replacement procedure codes would be assigned.
What is root operation?
When a device is completely removed without replacing it, the root operation is removal. For example, the removal of a tracheostomy tube or feeding tube represents such a procedure. There is an exception to this rule that involves replacing a previously placed device. A removal procedure is coded for taking out a device that was used in a previous replacement procedure; in other words, a complete re-do. If the previously placed device is completely removed and replaced, both removal and replacement procedure codes would be assigned. By coding both procedures, the data is reported with the capacity to illustrate that the latter procedure is actually what is defined in ICD-9-CM as a revision.
What is a replacement procedure?
In a replacement procedure, the objective is to replace the body part or a portion of the body part. This seems pretty straightforward. A caveat to remember is that if the code for replacement is assigned, the replacement code also captures the removal of the body part being replaced, and as such the removal or excision of the body part is not coded separately. A joint replacement, a bone graft, and a free skin graft are examples of replacement procedures.
Can ICD-10 PCS root operations be assigned correctly?
Based on theory, it would seem that ICD-10-PCS root operations could be assigned correctly with relative ease; however, practical application sometimes intersects with coding scenarios that make one question the selection of the appropriate root operation.
What is the ICd 9 code for knee replacement?
In ICD-9-CM, the Alphabetic main term entry Revision, subterms knee replacement, total (all components) identifies code 00.80. The code descriptor for 00.80 is Revision of knee replacement, total (all components) and is categorized under 00.8, Other knee and hip procedures. ICD-9-CM also provides codes for revision of tibial component only (00.81), revision of femoral component only (00.82), and revision of patellar component only (00.83). If revision of two knee components is performed then the coding professional would code the appropriate two component codes. ICD-9-CM does not differentiate laterality. Therefore, the code would be the same if performed on the left knee rather than the right knee. No additional code is assigned to remove the original knee prosthesis.
What is the correct root operation for ICd 10 PCS?
The correct root operation for this procedure in ICD-10-PCS is Revision as the objective of this procedure is to correct, to the extent possible, the dislodged or displaced lead. The Alphabetic Index main term is Revision of device in, Heart, which directs the coding professional to Table 02W. The ICD-10-PCS procedure code for this procedure is 02WA3MZ. Similar to ICD-9-CM, the ICD-10-PCS code for this procedure is used for the revision of any cardiac lead. The fifth character for the approach does provide distinct values for the various approaches used to perform this procedure. In this case, the fifth character is assigned the value of 3, identifying a percutaneous approach.
What is the ICD-10 code for tracheostomy tube?
The Index main term entry is Change device in, Trachea, which directs the coding professional to Table 0B2. The ICD-10-PCS code for this procedure is 0B21XFZ. The fourth character (1) identifies the body part as the trachea and the fifth character (X) identifies the approach or technique used to reach the operative site as external. The sixth character (F) identifies the device left at the operative site as a tracheostomy device.
What is the ICd 9 code for reposition of leads?
In ICD-9-CM, the Alphabetic Index main term Reposition, subterms, cardiac pacemaker, electrodes identifies code 37.75. The code descriptor for 37.75 is Revision of leads (electrodes) and is categorized under category 37, Other operations on heart and pericardium. This code is used to revise leads for various types of pacemakers and defibrillators. Additionally, ICD-9-CM does not provide distinct codes for the various approaches used to perform this procedure.
How many root operations are there in ICD-10?
In this article the Journal of AHIMA continues its 10-part Coding Notes series focusing on the 31 root operations in the Medical and Surgical section of ICD-10-PCS. This article will take a more in-depth look at the definitions and applications of the following three root operations:
What is a revision root operation?
The definition for the Revision root operation provided in the 2014 ICD-10-PCS Reference Manual is “Correcting, to the extent possible, a malfunctioning or displaced device.” The root operation Revision is coded when the objective of the procedure is to correct the position or function of a previously placed device, without taking the entire device out and putting in a whole new device in its place. Revision can include correcting a malfunctioning device by taking out and/or putting in part, but not all, of the device.
What is root operation change?
The definition for the Change root operation provided in the 2014 ICD-10-PCS Reference Manual is “Taking out or off a device from a body part and putting back an identical or similar device in or on the same body part without cutting or puncturing the skin or a mucous membrane.” The root operation Change represents only those procedures where a similar device is exchanged without making a new incision or puncture.
Popular Posts:
- 1. icd 10 code for shoulder
- 2. icd 9 code for hepatitis c with cirrhosis
- 3. icd 10 code for canabis use disorder
- 4. icd 10 code for recurrent oral ulcers
- 5. icd-10 code for hearing loss left ear
- 6. dsm v code for icd 10 code: f43.9
- 7. icd 10 code for chip fracture wrist
- 8. icd 10 code for sscd
- 9. icd 10 code for alcohol abuse and dependence
- 10. icd 9 code for diaper rash unspecified