Other specific joint derangements of right wrist, not elsewhere classified. M24. 831 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
Full
AnswerWhat is the ICD 10 code for ulnar impaction syndrome?
Ulnar impaction syndrome. ICD-10-CM M25.839 is grouped within Diagnostic Related Group (s) (MS-DRG v38.0): 555 Signs and symptoms of musculoskeletal system and connective tissue with mcc. 556 Signs and symptoms of musculoskeletal system and connective tissue without mcc. Convert M25.839 to ICD-9-CM.
What is the ICD 10 code for lesion of the ulnar nerve?
Lesion of ulnar nerve, right upper limb. G56.21 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2020 edition of ICD-10-CM G56.21 became effective on October 1, 2019. This is the American ICD-10-CM version of G56.21 - other international versions of ICD-10 G56.21 may differ.
What is the ICD 10 code for ulnar neuropathy of right arm?
Ulnar nerve syndrome Ulnar neuropathy of right arm ICD-10-CM G56.21 is grouped within Diagnostic Related Group (s) (MS-DRG v38.0): 073 Cranial and peripheral nerve disorders with mcc
What are the treatment options for ulnar impaction syndrome?
The most common surgical options to treat ulnar impaction syndrome (after physical therapy or other modalities have failed) include an ulnar shortening osteotomy (25390, Osteoplasty, radius or ulna; shortening) and hemiresection arthroplasty (25442, Arthroplasty with prosthetic replacement; distal ulna ).
What is the ICD-10 code for ulnar impaction syndrome?
The best choice is 718.83 (Unspecified derangement of joint; forearm) to represent instability. Ulnar impaction syndrome is also known as ulnar abutment syndrome, and can be a common complication after distal radial fracture.
What is ulnar impaction syndrome?
What is Ulnar Impaction Syndrome? Ulnar impaction syndrome occurs when the ulna is relatively larger than it should be when compared to the radius. This forces the ulna to bear more of the weight and force to the wrist on that side of the arm.
What is the ICD-10 code for ulnar minus variance?
2022 ICD-10-CM Diagnosis Code M24. 832: Other specific joint derangements of left wrist, not elsewhere classified.
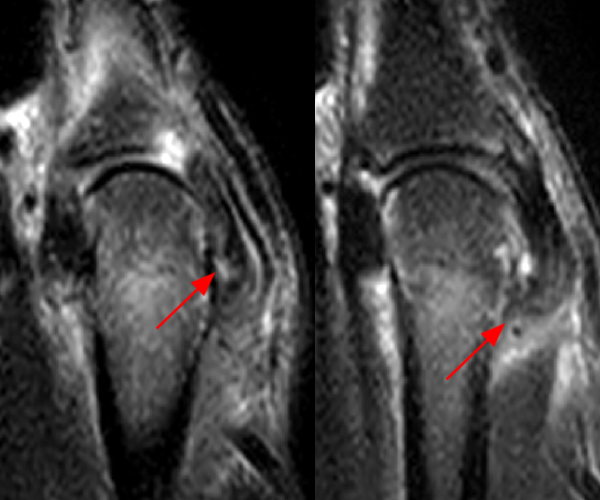
What does ulnar impaction syndrome look like?
Common symptoms are: pain, occasional edema, decreased wrist range of motion, decreased forearm rotation, and tenderness to palpation dorsally just distal to the ulnar head and just volar to the ulnar styloid process. The symptoms are commonly aggravated by forceful grip, forearm pronation, and ulnar deviation.
How do you get ulnar impaction syndrome?
Ulnar impaction syndrome is a progressive degenerative condition, most commonly resulting from repetitive abutment of a lengthened ulna, with the TFCC, lunate, triquetrum, and lunotriquetral ligament.
Where is the ulnar side of the wrist?
The ulnar side of your wrist is the side of your “pinkie” finger (or small finger), and pain on this side can be very common.
What does ulnar variance mean?
Ulnar variance, also known as Hulten variance, refers to the difference in height between the joint surfaces of the distal radius and ulna.
What is ulnar positive wrist?
Positive ulnar variance describes where the distal articular surface of the ulna is more than 2.5mm distal to the articular surface of the radius. It plays important role in wrist pathology such as ulnar impaction syndromes and thinning of the triangular fibrocartilage complex.
What is ulnar minus?
Negative ulnar variance is a condition in which the ulna is relatively shorter than the radius at the carpus. It was found in 21% of 203 normal wrists.
How rare is ulnar impaction syndrome?
Studies suggest that between 3 and 9% of all sports injuries involve the wrist and/or hand. Andrew Hamilton looks at ulnar impaction, one of the more common injuries to affect this region, especially among older athletes.
How is ulnar impaction treated?
Ulnar abutment syndrome can be treated by a variety of nonsurgical and surgical methods. These range from anti-inflammatory medications, immobilization, and corticosteroid injections to TFCC debridement, ulnar shortening osteotomies, and arthroscopic wafer procedures.
Where is the ulnar nerve in the arm?
The ulnar nerve runs behind the medial epicondyle on the inside of the elbow. Beyond the elbow, the ulnar nerve travels under muscles on the inside of your forearm and into your hand on the side of the palm with the little finger.
How to measure ulnar variance?
Measured by drawing a transverse line at the level of the lunate fossa and a second transverse line at the level of the ulnar head, and determining the distance between the two lines. Positive ulnar variance increases with power grip and pronation. Consider pronated grip view. (Tomaino MM, J Hand Surg 2000;25Am:352). Normal = neutral (articular surface of distal ulna and radius equal). Postive (ulna longer) associated with ulnocarpal impaction, lunotriquetral ligament injurie and TFCC tears. Negative (ulna shorter) associated with carpal instability, Keinbock's disease.
What is the ulnolunate abutment?
Ulnolunate abutment is between the ulnar articular seat and the lunte. Ulnotriquetral abutment is between the ulnar styloid and the triquetrum. Ulnocarpal Impaction Syndrome Anatomy. Load bearing across the wrist: 82% radius, 18% ulna in neutral postion.

Popular Posts:
- 1. icd 10 code for d72.829
- 2. icd 10 code for nonproliferative diabetic retinopathy
- 3. icd 10 code for unsp viral hep c wo coma
- 4. icd 9 cm code for acid reflux
- 5. icd 10 code for chorioamnionitis complicating delivery
- 6. icd 10 code for presence of blood clots
- 7. icd 10 code for rule out labor
- 8. icd 10 code for f88
- 9. icd 10 code for local reaction to bee venom right index finger
- 10. icd 10 code for chronic venous thromboembolism