Pressure ulcer of other site, stage 3. L89.893 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2019 edition of ICD-10-CM L89.893 became effective on October 1, 2018.
Pressure ulcer of other site, stage 3
The 2022 edition of ICD-10-CM L89. 893 became effective on October 1, 2021. This is the American ICD-10-CM version of L89.What is the ICD 10 code for diabetes mellitus with ulcer?
Type 2 diabetes mellitus with other skin ulcer. E11.622 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the ICD 10 code for pressure ulcer Stage 3?
Pressure ulcer stage 3 of right lower leg Pressure ulcer stage 3 of toes ICD-10-CM L89.893 is grouped within Diagnostic Related Group (s) (MS-DRG v38.0): 573 Skin graft for skin ulcer or cellulitis with mcc
What is the ICD 10 code for type 2 diabetes mellitus?
Type 2 diabetes mellitus with other skin ulcer. E11.622 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2020 edition of ICD-10-CM E11.622 became effective on October 1, 2019.
What is the ICD 10 code for non-pressure Chronic ulcer?
Non-pressure chronic ulcer of lower limb, not elsewhere classified L97- >. ICD-10-CM Diagnosis Code I87.03 ICD-10-CM Diagnosis Code I83.0 ICD-10-CM Diagnosis Code I83.2 A type 2 excludes note represents "not included here". A type 2 excludes note indicates that the condition excluded is not part of the condition it is excluded from...
What is the ICD-10 code for stage 3 Pressure ulcer?
Pressure ulcer of unspecified site, stage 3 L89. 93 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM L89. 93 became effective on October 1, 2021.
How do you code a diabetic ulcer?
621, E13. 622).” Of these options, the most commonly used codes for diabetic foot ulcers are E10. 621 (Type 1 diabetes mellitus with foot ulcer) and E11.
What is the ICD-10 code for diabetic leg ulcer?
ICD-10 Code for Type 2 diabetes mellitus with foot ulcer- E11. 621- Codify by AAPC.
What is the ICD-10 code for stage 3 sacral ulcer?
ICD-10 code L89. 153 for Pressure ulcer of sacral region, stage 3 is a medical classification as listed by WHO under the range - Diseases of the skin and subcutaneous tissue .
Are diabetic ulcers considered pressure ulcers?
Diabetic ulcers may look similar to pressure ulcers; however, it is important to note that they are not the same thing. As the name may imply, diabetic ulcers arise on individuals who have diabetes, and the foot is one of the most common areas affected by these skin sores.
What is a diabetic pressure ulcer?
Diabetic foot and pressure ulcers are chronic wounds by definition. They share similar pathogeneses; i.e., a combination of increased pressure and decreased angiogenic response. Neuropathy, trauma, and deformity also often contribute to development of both types of ulcers.
What is the ICD-10 code for type 2 diabetes?
ICD-Code E11* is a non-billable ICD-10 code used for healthcare diagnosis reimbursement of Type 2 Diabetes Mellitus. Its corresponding ICD-9 code is 250. Code I10 is the diagnosis code used for Type 2 Diabetes Mellitus.
What is the ICD-10 code for diabetes?
E08. 3531 Diabetes mellitus due to underlying condition... E08. 3532 Diabetes mellitus due to underlying condition...
What is code e11621?
621 Type 2 diabetes mellitus with foot ulcer.
What is a Stage 3 pressure ulcer?
Stage 3 bedsores (also known as stage 3 pressure sores, pressure injuries, or decubitus ulcers) are deep and painful wounds in the skin. They are the third of four bedsore stages. These sores develop when a stage 2 bedsore penetrates past the top layers of skin but has yet not reached muscle or bone.
What is the code for pressure ulcer of sacral region Stage 3?
153 - Pressure ulcer of sacral region, stage 3.
What is the ICD-10 code for sacral decubitus ulcer?
159 for Pressure ulcer of sacral region, unspecified stage is a medical classification as listed by WHO under the range - Diseases of the skin and subcutaneous tissue .
What is a diabetic foot ulcer?
Regarded as the most common reason for hospital stays among people with diabetes, a diabetic foot ulcer (DFU) is an open sore caused by neuropathic (nerve) and vascular (blood vessel) complications of the disease. Typically located on the plantar surface, or bottom/top of toes, pad of foot, or heel of foot, these complex, ...
What is a L97.91 ulcer?
L97.91 -Non-pressure chronic ulcer of unspecified part of right lower leg. L97.92 – Non-pressure chronic ulcer of unspecified part of left lower leg. According to the American Podiatric Medical Association, about 14 to 24 percent of Americans with diabetic foot ulcers have amputations.
What are the risk factors for ulcers?
The most common risk factors for ulcer formation include – diabetic neuropathy, structural foot deformity, kidney disease, obesity and peripheral arterial occlusive disease. The condition can be effectively prevented if the underlying conditions causing it are diagnosed early and treated correctly.
How many amputations are there for diabetics?
The risk of foot ulceration and limb amputations increases with age and duration of diabetes. In the United States, about 82,000 amputations are performed each year on persons with diabetes; half of those ages 65 years or older. Treatment for diabetic foot ulcers varies depending on their causes.
How many people with diabetes have foot ulcers?
According to the American Podiatric Medical Association (APMA), approximately 15 percent of people with diabetes suffer from foot ulcers. Of those who develop a foot ulcer, about 6 percent will be hospitalized due to serious infections or other ulcer-related complications.
Where does neuropathic ulcer occur?
Neuropathic ulcers– occur where there is peripheral diabetic neuropathy, but no ischemia caused by peripheral artery disease. This type of foot infection generally occurs on the plantar aspect of the foot under the metatarsal heads or on the plantar aspects of the toes.
Where are diabetic ulcers located?
Typically located on the plantar surface, or bottom/top of toes, pad of foot, or heel of foot , these complex, chronic wounds can affect people with both Type 1 and Type 2 diabetes. If left untreated, diabetic foot ulcers can have a permanent, long-term impact on the morbidity, mortality and quality of a patients’ life.
What is the L89 code for a pressure ulcer?
Pressure injuries with skin breakdown are considered pressure ulcers. An additional L89 code specifies the stage (depth of tissue injury) and the anatomical site. Pressure ulcers form in sites that experience shear or pressure, typically in tissue overlying bony prominences such as elbows, the sacrum, hips, or heels.
Why do diabetics get ulcers?
The American Podiatric Medical Association adds that “ (diabetic foot) ulcers form due to a combination of factors , such as lack of feeling in the foot, poor circulation, foot deformities, irritation (such as friction or pressure), and trauma, as well as duration of diabetes .”. They go on to note that “vascular disease can complicate a foot ulcer, ...
What percentage of diabetics have neuropathy?
After 10 years, ~90 percent of Type 1 and Type 2 diabetics have some degree of neuropathy, most commonly affecting the feet and legs, and 90 percent of diabetic foot ulcers have diabetic neuropathy as a contributing factor. If the diabetic doesn’t recognize discomfort due to nerve impairment, they may not adjust their shoes ...
What causes diabetic foot ulcers?
A “diabetic foot ulcer,” which is caused exclusively by hyperglycemia, in the absence of neuropathy or ischemia, is a rarity. That term almost always refers to an ulcer on the foot of a diabetic that derives from neuro/ischemic etiology, as opposed to being strictly and principally due to pressure injury.
What happens when blood sugar is low?
Poorly controlled blood sugars weaken the small blood vessel walls and predispose patients to arteriosclerosis. This impairs the circulation and causes ischemia of the soft tissues, especially of the lower extremities. Many diabetics have both diabetic peripheral neuropathy and angiopathy.
Why are pressure ulcers considered a patient safety indicator?
Pressure ulcers are deemed patient safety indicators and hospital acquired conditions because a concerted program for prevention and treatment can prevent them and protect our patients from iatrogenic harm. The diagnosis of a “pressure ulcer” may trigger prevalence and incident reporting.
Can diabetes cause heel ulcers?
Heel ulcers, however, are usually a consequence of a pressure injury, although it is also possible to have another mechanism cause a non-pressure injury involving the heel. Diabetes may accelerate or complicate the injury. Neuropathy results in malum perforans pedis (a.k.a. bad perforating foot) ulcers.
What are the stages of pressure ulcers?
ICD-10 Code Assignment for Pressure/Non Pressure Ulcers 1 Stage 1: Skin changes limited to persistent focal edema 2 Stage 2: An abrasion, blister, and partial thickness skin loss involving the dermis and epidermis 3 Stage 3: Full thickness skin loss involving damage and necrosis of subcutaneous tissue 4 Stage 4: Necrosis of soft tissues through the underlying muscle, tendon, or bone 5 Unstageable: Based on clinical documentation the stage cannot be determined clinically (e.g., the wound is covered with eschar) or for ulcers documented as deep tissue injury without evidence of trauma.
What stage of ulcers are there on the elbow?
The pressure ulcers on the elbows are documented as partial thickness into the dermis, which supports stage 2 (stated to be healing or abrasion, blister, partial thickness skin loss involving epidermis and/or dermis)—which again matches the physician documentation.
What is ulcer depth?
Ulcer depth: with necrosis of muscle. with muscle involvement without evidence of necrosis. The Grade 3 foot has ulcer with deep abscess, osteitis or osteomyelitis, pyarthrosis, plantar space abscess, or infection of the tendon and tendon sheaths.
What is a grade 2 foot?
The Grade 2 foot has a lesion that is deeper and extends to the bone, ligament, tendon, joint capsule or deep fascia. There is yet no abscess or osteomyelitis. The Grade 3 foot has ulcer with deep abscess, osteitis or osteomyelitis, pyarthrosis, plantar space abscess, or infection of the tendon and tendon sheaths.
Terminology

Shear and pressure are the mechanisms that lead to what are known as pressure injuries. In 2016, the National Pressure Ulcer Advisory Panel (NPUAP) recommended transitioning to the terminology of pressure injury because although underlying tissue may be damaged, overlying skin may appear intact. Pressure inj…
Diagnosis
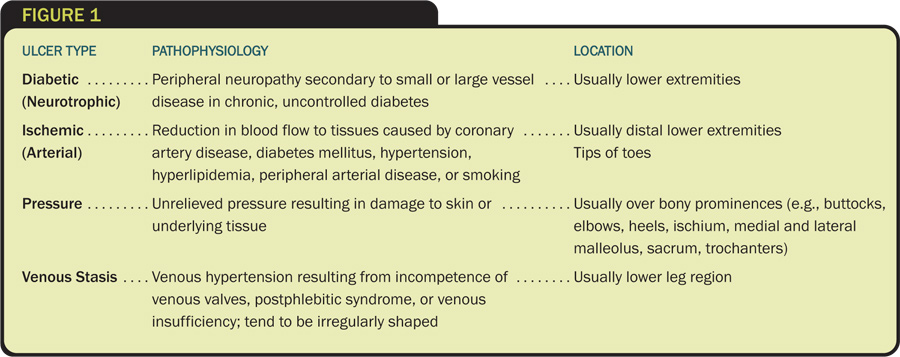
- There are medical diagnoses that predispose patients to develop secondary conditions. Diabetes mellitus is a pervasive endocrinopathy whereby hyperglycemia affects every organ and system in the body, including the nerves and blood vessels. It makes a patient more prone to infection and poor healing. Diabetics are prone to foot ulcers, often with contributions from neuropathic, ische…
Clinical significance
- Diabetics also often have diseases of both large and small arteries. Poorly controlled blood sugars weaken the small blood vessel walls and predispose patients to arteriosclerosis. This impairs the circulation and causes ischemia of the soft tissues, especially of the lower extremities.
Causes
- Heel ulcers, however, are usually a consequence of a pressure injury, although it is also possible to have another mechanism cause a non-pressure injury involving the heel. Diabetes may accelerate or complicate the injury. The American Podiatric Medical Association adds that (diabetic foot) ulcers form due to a combination of factors, such as lack of feeling in the foot, po…
Signs and symptoms
- Neuropathy results in malum perforans pedis (a.k.a. bad perforating foot) ulcers. These are painless, non-necrotic, circular lesions circumscribed by hyperkeratosis. They often overlie a metatarsal head. Ischemic wounds manifest local signs of ischemia such as thin, shiny, hairless skin with pallor and coldness. These are often found at areas of friction and may be painful.
Epidemiology
- The American Orthopaedic Foot & Ankle Society states that ulceration is an extremely common complication in diabetic patients (up to 12 percent of the population). The plantar surface is the most common site of ulceration, especially at areas of bony prominence. The Society also points out that the presence of neuropathy is the key factor in development of diabetic ulceration.
Society and culture
- In the podiatric literature, NPUAP is often referenced as having given guidance to use diabetic foot ulcer for any ulcer on the foot of a diabetic, even if arterial disease and/or pressure played a role in its development. I think this is simplistic and derived from literature not aimed at physicians/APPs. It is common in the literature to see the term diabetic foot ulcer used for all-co…
Treatment
- Ultimately, the clinical concern is to treat the lesion appropriately, regardless of the name attached to it. The treatment for both pressure ulcers and diabetic foot ulcers includes offloading (i.e., pressure mitigation, often by means of padding, shoe modifications, contact casts, boots, or non-weight-bearing strategies). Any non-healing wound should be assessed for neuropathy and …
Popular Posts:
- 1. icd 10 code for necituria
- 2. icd 10 code for obstructed jejunostomy tube
- 3. icd 10 code for left tka infection
- 4. 2017 icd 10 code for anemia secondary to a malignant neoplasm of her throat
- 5. icd-10 code for mri lumbar spine
- 6. icd 10 code for infant colic
- 7. icd 10 code for dislocation of right ankle joint
- 8. icd 10 code for decreased wbcs
- 9. icd 10 code for antral erosions
- 10. icd 10 code for k58.00