ICD-10-PCS is intended to replace ICD-9 volume 3 for facility reporting of inpatient procedures. Current Procedural Terminology (CPT) is still used for all outpatient procedures. Healthcare Common Procedural Coding System (HCPCS) is still used as before.
ICD-10
The International Classification of Diseases (ICD) is a globally used diagnostic tool for epidemiology, health management and clinical purposes. The ICD is maintained by the World Health Organization (WHO), which is the directing and coordinating authority for health within the United Nations System.
https://en.wikipedia.org › wiki › International_Classification_o...
What are PCS codes used for?
- 06.11, Closed [percutaneous] [needle] biopsy of thyroid gland (10 codes)
- 06.12, Open biopsy of thyroid gland (5 codes)
- 06.13, Biopsy of parathyroid gland (36 codes)
- 06.19, Other diagnostic procedures on thyroid and parathyroid glands (22 codes) and cover procedure types (operations) including Drainage, Excision, Inspection, and Revision.
How to ICD 10 PCs code Hartmann's procedure?
large bowel (Hartmann’s procedure). • Procedural steps: – Divide the bowel proximal to the area of concern. – Create a circular opening through the abdominal wall. – Pull the proximal end of the divided bowel through the abdominal wall opening.
What are ICD 10 codes lookup?
The ICD-10-CM is a catalog of diagnosis codes used by medical professionals for medical coding and reporting in health care settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates.
What is a valid ICD 10 code?
The following 72,752 ICD-10-CM codes are billable/specific and can be used to indicate a diagnosis for reimbursement purposes as there are no codes with a greater level of specificity under each code. Displaying codes 1-100 of 72,752: A00.0 Cholera due to Vibrio cholerae 01, biovar cholerae. A00.1 Cholera due to Vibrio cholerae 01, biovar eltor. A00.9 Cholera, unspecified.
In what setting should ICD-10-PCS codes be used?
inpatient settingICD-10-PCS is a classification system which is used for coding procedures and services provided in the inpatient setting of hospitals in the United States.
What does ICD-10-PCS stand for?
The International Classification of Diseases 10th Revision Procedure Coding System (ICD-10-PCS) has been developed as a replacement for Volume 3 of the International Classification of Diseases 9th Revision (ICD-9-CM). The development of ICD-10-PCS was funded by the U.S. Centers for Medicare and Medicaid Services (CMS).
What is the purpose of ICD PCS and CPT codes?
ICD-10-CM diagnosis codes provide the reason for seeking health care; ICD-10-PCS procedure codes tell what inpatient treatment and services the patient got; CPT (HCPCS Level I) codes describe outpatient services and procedures; and providers generally use HCPCS (Level II) codes for equipment, drugs, and supplies for ...
What are ICD-10-PCS tables?
The ICD-10-PCS Tables contains all valid codes in table format. The tables are arranged in alphanumeric order, and organized into separate tables according to the first three characters of the seven-character code.
Why is ICD-10-PCS important?
Improved quality of data. The granularity of ICD-10-CM and ICD-10-PCS is vastly improved over ICD-9-CM and will enable greater specificity in identifying health conditions. It also provides better data for measuring and tracking health care utilization and the quality of patient care.
What does PCS stand for medical coding?
The International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) is a U.S. cataloging system for procedural codes that track various health interventions taken by medical professionals.
Do physicians use ICD-10-PCS?
A: No. ICD-10 procedure codes will only be used for facility reporting of hospital inpatient services. Current Procedural Terminology (CPT®) codes will continue to be used for physician and outpatient services.
Who maintains ICD-10-PCS?
The ICD-10-PCS code set is not used internationally and is maintained by the Centers for Medicare and Medicaid Services (CMS).
What is the role of ICD-10-PCS according to the Uhdds guidelines?
One of the sources that hospital inpatient facilities use to define the facility-specific ICD-10-PCS procedure requirements is the Uniform Hospital Discharge Data Set (UHDDS) reporting criteria. The UHDDS guidelines are used by hospitals to report inpatient data elements in a standardized manner.
What is PCS table?
The ICD-10-PCS Tables contains all valid codes in table format. The tables are arranged in alphanumeric order, and organized into separate tables according to the first three characters of the seven-character code.
How many sections are there in ICD-10-PCS?
17 sectionsProcedures are divided into 17 sections that relate to the type of procedure (see “Sections of ICD-10-PCS,” below, left). The first character of the procedure code identifies the section.
How do I find the ICD-10-PCS code?
ICD10Data.com is a free reference website designed for the fast lookup of all current American ICD-10-CM (diagnosis) and ICD-10-PCS (procedure) medical billing codes.
What is difference between ICD and CPT codes?
CPT codes refer to the treatment being given, while ICD codes refer to the problem that the treatment is aiming to resolve. The two work hand-in-hand to quickly provide payors specific information about what service was performed (the CPT code) and why (the ICD code).
Who maintains ICD-10-PCS?
The ICD-10-PCS code set is not used internationally and is maintained by the Centers for Medicare and Medicaid Services (CMS).
How many ICD-10 codes are there?
Another difference is the number of codes: ICD-10-CM has 68,000 codes, while ICD-10-PCS has 87,000 codes.
What is the ICd 10 PCS?
ICD-10-PCS was developed in the 1990s and covers the then-new technique of laparoscopic surgery. Common procedures now in use involving interventional radiology or robotics are not readily accommodated. The coding index shows that the accepted code for the insertion of a cardiac stent is a Dilation operation involving a Percutaneous Endoscopic approach but gives no indication of radiographic involvement. It is not clear that extending this analogy is appropriate for other interventional radiology procedures such as a repair of a brain aneurysm involving the placement of coils or needle aspirations under radiographic control. Similarly, new robotic devices are handled crudely in the Other Procedure (8) section only. Both would benefit by the introduction of new approaches or qualifiers.
When was the coding system developed?
The code system was developed in the 1990s, but use of the continually updated codes will start almost 20 years later. Outside of a pilot study focused on ease of use, little practical knowledge exists concerning the ease or efficacy of coding procedures in the code set.
What is the ICD-10 PCS code for bronchoscopy?
A bronchoscopy is a simple example. The basic code is 0BJ (1)8ZZ where (1) is for the deepest anatomical location explored during the procedure. It is assumed all locations above also were explored.
What are the codes for breast cancer?
For example 0, 1, and 2 are used for right, left and bilateral breast (s) respectively in Imaging and Radiation Oncology, while the codes T, U and V are used in Medical and Surgical.
Is CPT still used?
Current Procedural Terminology (CPT) is still used for all outpatient procedures. Healthcare Common Procedural Coding System (HCPCS) is still used as before. Common procedures that are not unique to the inpatient setting, such as laboratory tests and educational sessions, were omitted from PCS.
Why do I prefer PCS or CPT?
There are a few reasons why I prefer PCS coding. One is because CPT® codes are rarely as specific as PCS codes: For any given procedure, CPT® generally offers one or two codes compared to the multiple codes PCS offers .#N#For example, as shown in Figure A, a total abdominal hysterectomy with bilateral salpingo-oopherectomy (TAHBSO) in CPT® is coded 58150 Total abdominal hysterectomy (corpus and cervix), with or without removal of tube (s), with or without removal of ovary (s); which is not specific as to whether one or both ovaries and fallopian tubes were removed.#N#In PCS, as shown in Figure B, a TAHBSO is four codes (0UT90ZZ, 0UTC0ZZ, 0UT20ZZ, 0UT70ZZ), allowing you to specify the uterus and cervix were completely removed, as well as bilateral ovaries and bilateral fallopian tubes, and that it was an open procedure, not laparoscopic. There are different codes for when only one ovary or fallopian tube is removed, and they are also specific to laterality.
How to use index in PCS?
The simplest way to use the index in PCS is to first look up the defined root operation. From there, it’s easy to find what options are available for that procedure. If you start with the section or even the body system, it’s more difficult and takes more time.#N#Example: Laparoscopic cholecystectomy.#N#Look up the root operation Resection (the entire gallbladder is being removed). Then search for the body part, Gallbladder (0FT4). Next, determine whether the approach was laparoscopic/percutaneous endoscopic or open. There is no device or qualifier available for this procedure, so No Device (Z) and No Qualifier (Z) are the only choices.#N#Some encoders will let you just start with “cholecystectomy” and lead you into Excision – Cutting out or off, without replacement, a part/portion of the body part vs. R esection – Cutting out or off, without replacement, all of a body part, then Open vs. Laparoscopic. As shown in Figure G, the valid code for laparoscopic cholecystectomy is 0FT44ZZ.#N#The tables show you what options are available for the approach, as well as other characters (body part, device, qualifier) for a given operation (excision, resection, etc.), per the body part the surgery is performed on. For the gallbladder resection, you can see in Figure H, the options for Via Natural or Artificial Opening and V ia Natural or Artificial Opening Endoscopic are grayed out, as they are not available approaches for that body part and procedure.#N#There is no reason to feel overwhelmed when it comes to ICD-10-PCS coding. If you familiarize yourself with the PCS coding guidelines, particularly with previous inpatient coding knowledge and pursue continued education, you’ll find assigning PCS codes easier than expected.
What is the fifth character of a PCS code?
Approach is the fifth character of a PCS code and is the “technique” the physician. used to reach the site of the procedure. There are seven approaches to choose. Not all. approaches are available for each procedure. As shown in Figure F, the procedure.
How many characters are in an ICD-10 code?
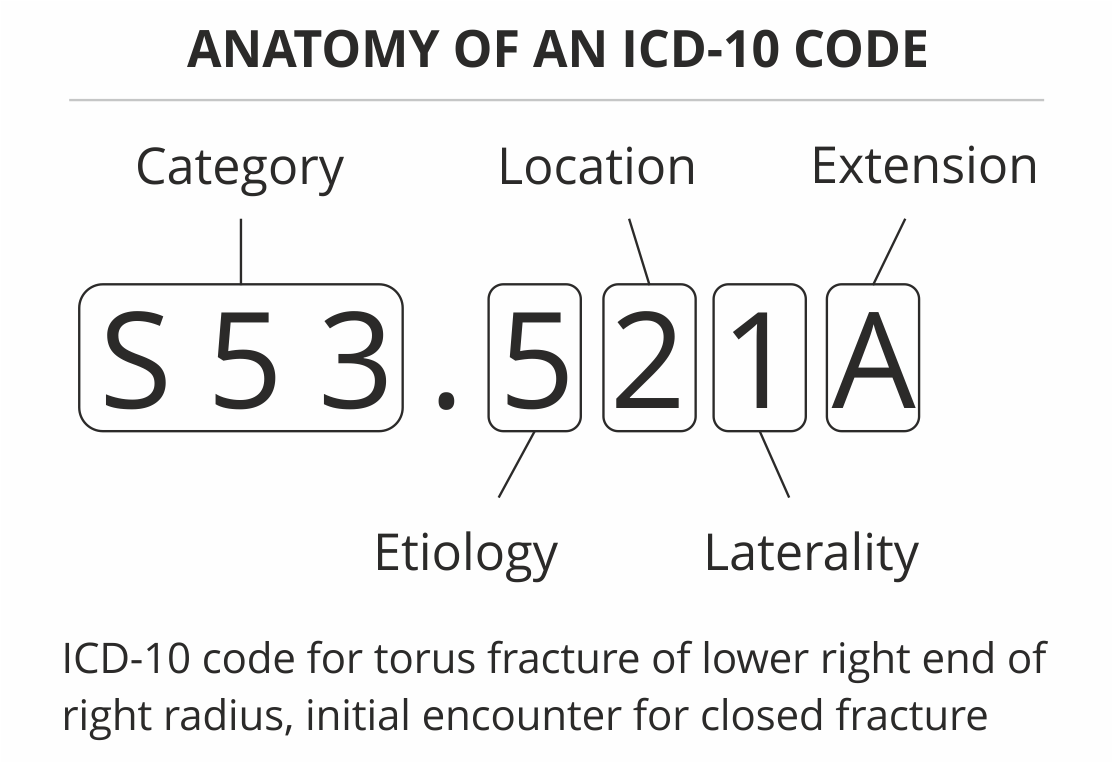
A1 ICD-10-PCS codes are composed of seven characters. Each character is an axis of classification that specifies information about the procedure performed. Within a defined code range, a character specifies the same type of information in that axis of classification.
When is a device coded?
General guidelines B6.1a A device is coded only if a device remains after the procedure is completed. If no device remains, the device value No Device is coded. In limited root operations, the classification provides the qualifier values Temporary and Intraoperative, for specific procedures involving clinically significant devices, where the purpose of the device is to be utilized for a brief duration during the procedure or current inpatient stay. If a device that is intended to remain after the procedure is completed requires removal before the end of the operative episode in which it was inserted (for example, the device size is inadequate or a complication occurs), both the insertion and removal of the device should be coded.
What is section X code?
When section X contains a code title which fully describes a specific new technology procedure, and it is the only procedure performed , only the section X code is reported for the procedure. There is no need to report an additional code in another section of ICD-10-PCS. Example: XW04321 Introduction of Ceftazidime-Avibactam Anti-infective into Central Vein, Percutaneous Approach, New Technology Group 1, can be coded to indicate that Ceftazidime-Avibactam Anti-infective was administered via a central vein. A separate code from table 3E0 in the Administration section of ICD-10-PCS is not coded in addition to this code.
What is B4.1A code?
General guidelines B4.1a If a procedure is performed on a portion of a body part that does not have a separate body part value, code the body part value corresponding to the whole body part.
When to use B2.1A?
General guidelines B2.1a The procedure codes in Anatomical Regions, General, Anatomical Regions, Upper Extremities and Anatomical Regions, Lower Extremities can be used when the procedure is performed on an anatomical region rather than a specific body part, or on the rare occasion when no information is available to support assignment of a code to a specific body part.

The Basics
- ICD-10-PCS is intended to replace ICD-9 volume 3 for facility reporting of inpatient procedures. Current Procedural Terminology (CPT) is still used for all outpatient procedures. Healthcare Common Procedural Coding System (HCPCS) is still used as before. Common procedures that are not unique to the inpatient setting, such as laboratory tests and ed...
An Overview of Use
- Although the Centers for Medicare and Medicaid Services has developed crosswalks from ICD-9 volume 3 to ICD-10-PCS, they are not intended for direct use in coding. The varied assignments for each axis make code such matching difficult. For example, the volume 3 code 06.1 (Diagnostic procedures on thyroid and parathyroid glands) corresponds to 73 codes in ICD-10-PCS: 1. 06.11…
Coding Parts
- Many procedures are composed of multiple parts, and ICD-10-PCS has specific, and sometimes complex, rules regarding how to code these. A bronchoscopy is a simple example. The basic code is 0BJ(1)8ZZ where (1) is for the deepest anatomical location explored during the procedure. It is assumed all locations above also were explored. A bit more complex is a partial thyroidectomy. …
Coding The Whipple
- Pancreaticoduodenectomy, commonly called a Whipple procedure, is a complex surgical procedure involving multiple abdominal organs. It has a unique ICD-9 code of 52.7. It has no corresponding ICD-10-PCS code. The procedure be best described by multiple ICD-10-PCS codes representing the specific organ parts that are excised, as no organ is totally removed (a resectio…
Coding New Methods
- ICD-10-PCS was developed in the 1990s and covers the then-new technique of laparoscopic surgery. Common procedures now in use involving interventional radiology or robotics are not readily accommodated. The coding index shows that the accepted code for the insertion of a cardiac stent is a Dilation operation involving a Percutaneous Endoscopic approach but gives n…
Conclusion
- The preceding examples illustrate that selecting the correct PCS code requires a greater knowledge of anatomy and physiology than is required under ICD-9. The degree of new knowledge required will depend on the coder’s personal knowledge and the speciality areas he or she codes. Regardless, ICD-10-PCS terms differ from standard terminology enough that coders must crest …
Acknowledgements
- The author wishes to thank Claire Dixon-Lee, PhD, and Sue Bowman, RHIA, CCS, for their careful review of this article and thoughtful comments.
References
- Centers for Medicare and Medicaid Services. “2010 ICD-10-PCS and GEMs.”(Multiple resources.) Steindel, Steven J. “International Classification of Diseases, 10th edition, Clinical Modification and Procedure Coding System: Descriptive Overview of the Next Generation HIPAA Code Sets.”Journal of the American Medical Informatics Association17, no. 3 (May-June 2010): 274-82.
Popular Posts:
- 1. icd 10 code for afternoon
- 2. icd 10 code for vitreous degeneration bilateral
- 3. icd 10 code for proyalisis on right knee
- 4. icd 10 code for iufd
- 5. icd 10 code for hepatitis screening
- 6. icd 10 code for left basal ganglia infarct
- 7. icd-10-cm code for twins and which one is born and the other is stillborn
- 8. icd-10 code for follow-up after surgery
- 9. icd 10 code for multidrug overdose
- 10. icd 10 code for stress fracture right 5th metatarsal