A screening colonoscopy should be reported with the following International Classification of Diseases, 10th edition (ICD-10) codes: Z12. 11: Encounter for screening for malignant neoplasm of the colon .May 1, 2016
malignant neoplasm of the colon
Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum (parts of the large intestine). Signs and symptoms may include blood in the stool, a change in bowel movements, weight loss, and fatigue.
https://en.wikipedia.org › wiki › Colorectal_cancer
How do you code a screening colonoscopy?
Apr 11, 2020 · A screening colonoscopy should be reported with the following International Classification of Diseases, 10th edition (ICD-10) codes: Z12. 11: Encounter for screening for malignant neoplasm of the colon. Z80.
What is the procedure code for a colonoscopy?
45389 Colonoscopy, flexible, proximal to splenic flexure; with transendoscopic ultrasound guided intramural or transmural fine needle aspiration/biopsy (s) Diagnosis Codes: ICD-10 [Effective 10/1/15] Code Description D12.0 Benign neoplasm of cecum D12.1 Benign neoplasm of appendix D12.2 Benign neoplasm of ascending colon
How to code screening and diagnostic colonoscopy?
Oct 01, 2015 · The following ICD-10-CM codes have been added to the list of ICD-10-CM codes that support medical necessity, Group 1 codes: K50.00, K50.90, K51.90, K51.911, K51.912, K51.913, K51.914, and K51.918, in response to an external inquiry.
How do you code an incomplete colonoscopy?
Oct 01, 2015 · 2022 ICD-10-PCS Procedure Code 0DBN4ZX Excision of Sigmoid Colon, Percutaneous Endoscopic Approach, Diagnostic 2016 2017 2018 2019 2020 2021 2022 Billable/Specific Code ICD-10-PCS 0DBN4ZX is a specific/billable code that can be used to indicate a procedure. Code History 2016 (effective 10/1/2015): New code (first year of non …
What is the procedure code for colonoscopy?
45378Group 1CodeDescription45378COLONOSCOPY, FLEXIBLE; DIAGNOSTIC, INCLUDING COLLECTION OF SPECIMEN(S) BY BRUSHING OR WASHING, WHEN PERFORMED (SEPARATE PROCEDURE)45379COLONOSCOPY, FLEXIBLE; WITH REMOVAL OF FOREIGN BODY(S)45380COLONOSCOPY, FLEXIBLE; WITH BIOPSY, SINGLE OR MULTIPLE22 more rows
Are there ICD 10 procedure codes?
ICD-10-PCS will be the official system of assigning codes to procedures associated with hospital utilization in the United States. ICD-10-PCS codes will support data collection, payment and electronic health records. ICD-10-PCS is a medical classification coding system for procedural codes.
What is procedure code G0121?
--Code G0121 (colorectal cancer screening; colonoscopy on an individual not meeting criteria for high risk) should be used when this procedure is performed on a beneficiary who does NOT meet the criteria for high risk.
What is an ICD-10 diagnosis code?
Used for medical claim reporting in all healthcare settings, ICD-10-CM is a standardized classification system of diagnosis codes that represent conditions and diseases, related health problems, abnormal findings, signs and symptoms, injuries, external causes of injuries and diseases, and social circumstances.May 20, 2021
What is the difference between ICD-10 and ICD-10-PCS?
The main differences between ICD-10 PCS and ICD-10-CM include the following: ICD-10-PCS is used only for inpatient, hospital settings in the U.S., while ICD-10-CM is used in clinical and outpatient settings in the U.S. ICD-10-PCS has about 87,000 available codes while ICD-10-CM has about 68,000.
What is the ICD 10 code for incomplete colonoscopy?
Incomplete Colonoscopy B Incomplete Colonoscopies) are 44388, 45378, G0105, and G0121.Jul 8, 2021
What is diagnosis code Z86 010?
Personal history of colonic polyps“Code Z86. 010, Personal history of colonic polyps, should be assigned when 'history of colon polyps' is documented by the provider. History of colon polyp specifically indexes to code Z86. 010.” “AHA Coding Clinic, First Quarter 2017, there is not an Index entry for rectal polyps.
Why is a colonoscopy considered a diagnostic procedure?
A colonoscopy is considered diagnostic when you've had: Signs or symptoms in the lower gastrointestinal tract noted in your medical record before the procedure, including: Abdominal pain that doesn't improve.Jan 25, 2022
What is colonoscopy procedure?
Definition of Terms Colonoscopy: A colonoscopy is a procedure that permits the direct examination of the mucosa of the entire colon by using a flexible lighted tube. The procedure is done with sedation in a hospital outpatient department, in a clinic , or an office facility. During the colonoscopy a doctor can biopsy and remove pre – cancerous ...
What is a screening colonoscopy?
General definitions of procedure indications from various specialty societies , including the ACA: * A screening colonoscopy is done to look for disease, such as cancer, and treat early conditions, if indicated, in people without symptoms. * A diagnostic colonoscopy is done to confirm or rule out a condition in a person who is symptomatic ...
What is a provider policy?
A provider also can be a place where medical care is given, like a hospital, clinic, or lab.This policy informs them about when a service may be covered.
Is colonoscopy a screening test?
This guideline applies only to people of average risk. Colonoscopy is only one of the screening tests that can be used. This benefit coverage guideline provides general information about how the health plan decides whether a colonoscopy is covered under the preventive or diagnostic (medical) benefits.
General Information
CPT codes, descriptions and other data only are copyright 2020 American Medical Association. All Rights Reserved. Applicable FARS/HHSARS apply.
Article Guidance
This Billing and Coding Article provides billing and coding guidance for Local Coverage Determination (LCD) L33671 (Diagnostic Colonoscopy). Please refer to the LCD for reasonable and necessary requirements.
ICD-10-CM Codes that Support Medical Necessity
It is the provider’s responsibility to select codes carried out to the highest level of specificity and selected from the ICD-10-CM code book appropriate to the year in which the service is rendered for the claim (s) submitted
ICD-10-CM Codes that DO NOT Support Medical Necessity
All those not listed under the “ICD-10 Codes that Support Medical Necessity” section of this article.
Bill Type Codes
Contractors may specify Bill Types to help providers identify those Bill Types typically used to report this service. Absence of a Bill Type does not guarantee that the article does not apply to that Bill Type.
Revenue Codes
Contractors may specify Revenue Codes to help providers identify those Revenue Codes typically used to report this service. In most instances Revenue Codes are purely advisory. Unless specified in the article, services reported under other Revenue Codes are equally subject to this coverage determination.
What is the code for colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code Z12.11 ( encounter for screening for malignant neoplasm of the colon ).
What is a colonoscopy screening?
As such, “screening” describes a colonoscopy that is routinely performed on an asymptomatic person for the purpose of testing for the presence of colorectal cancer or colorectal polyps. Whether a polyp or cancer is ultimately found does not ...
What are the global periods for colonoscopy?
Typically, procedure codes with 0, 10 or 90-day global periods include pre-work, intraoperative work, and post-operative work in the Relative Value Units (RVUs) assigned . As a result, CMS’ policy does not allow for payment of an Evaluation and Management (E/M) service prior to a screening colonoscopy. In 2005, the Medicare carrier in Rhode Island explained the policy this way:
Does Medicare cover colonoscopy?
However, diagnostic colonoscopy is a test performed as a result of an abnormal finding, sign or symptom. Medicare does not waive the co-pay and deductible when the intent of the visit is to perform a diagnostic colonoscopy. Medicare waives the deductible but not the co-pay when a procedure scheduled as a screening is converted to a diagnostic ...
Is E/M covered by Medicare?
Medicare defines an E/M prior to a screening colonoscopy as routine, and thus non-covered. However, when the intent of the visit is a diagnostic colonoscopy an E/M prior to the procedure ordered for a finding, sign or symptom is a covered service.
What does PT mean in CPT?
The PT modifier ( colorectal cancer screening test, converted to diagnostic test or other procedure) is appended to the CPT ® code.
Can you remove polyps at screening colonoscopy?
It is not uncommon to remove one or more polyps at the time of a screening colonoscopy. Because the procedure was initiated as a screening the screening diagnosis is primary and the polyp (s) is secondary. Additionally, the surgeon does not report the screening colonoscopy HCPCS code, but reports the appropriate code for the diagnostic or therapeutic procedure performed, CPT ® code 45379—45392.
What is the ICD-10 code for colonoscopy without biopsy?
Point to note: Code 45378 is the base code for a colonoscopy without biopsy or other interventions. It includes brushings or washings if performed. Report 45378 with ICD-10 code Z86.010 on the first line of the CMS 1500 form.
What is the HCPCS code for colonoscopy?
For Medicare beneficiaries, screening colonoscopy is reported using the following HCPCS codes: - G0105 (Colorectal cancer screening; colonoscopy on individual at high risk), for a Medicare beneficiary at high risk for colorectal cancer, and the appropriate diagnosis code that necessitates the more frequent screening.
What is colonoscopy examination?
CPT defines a colonoscopy examination as "the examination of the entire colon, from the rectum to the cecum or colon-small intestine anastomosis, and may include an examination of the terminal ileum or small intestine proximal to an anastomosis" as well.
How often does Medicare require colonoscopy?
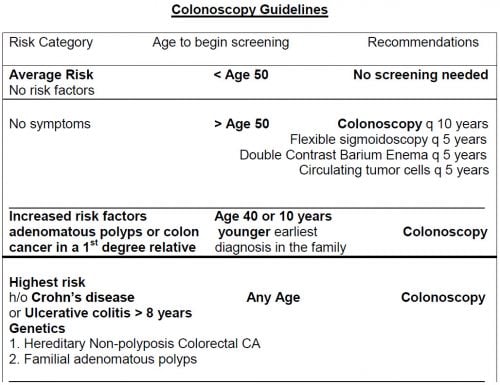
Medicare beneficiaries without high-risk factors are eligible for a screening colonoscopy every ten years. Beneficiaries at higher risk for developing colorectal cancer are eligible for screening once every 24 months. Medicare considers an individual who is at high risk of developing colorectal cancer as one who has one or more of the following:
What is a colonoscopy?
A Diagnostic colonoscopy is performed when an abnormal finding, sign, or symptom is found such as diarrhea, anemia, abdominal pain, or rectal bleeding. A Screening colonoscopy is performed on person without symptoms in order to test for the presence of colorectal cancer or colorectal polyps. Even if a polyp or cancer is found during ...
What modifier is used for colonoscopy?
53 - Medicare guidelines state that if a patient is scheduled for a screening colonoscopy, but because of poor prep the scope cannot be advanced beyond the splenic fixture, the procedure should be coded as a colonoscopy with modifier 53 (discontinued procedure).
How effective is colonoscopy?
According to a study by the American Cancer Society, 90% colorectal cancer (CRC) cases are detected in individuals with over 50 years in the U.S and colonoscopy is the most effective and the most commonly adopted procedure for the diagnosis and screening of CRC in older adults.

Popular Posts:
- 1. icd 10 code for carotid artery stenosis
- 2. icd 10 code for blood clot
- 3. icd 10 code for senile purpura
- 4. icd 10 cm code for rabies vaccine
- 5. icd 10 code for tingling in feet
- 6. icd 10 code for osteonecrosis of bilateral tibia
- 7. what is the icd 10 code for meniscal tear
- 8. icd 10 code for bilateral lateral epicondylitis
- 9. icd 10 code for left displaced patella fracture
- 10. procedural icd 10 code for mini maze