45.23 Colonoscopy - ICD-9-CM Vol.
What are the guidelines for a colonoscopy?
Jan 26, 2012 · ICD-9 Codes that Support Medical Necessity for colonoscopy procedures. 009.0 – 009.1 INFECTIOUS COLITIS ENTERITIS AND GASTROENTERITIS – COLITIS ENTERITIS AND GASTROENTERITIS OF PRESUMED INFECTIOUS ORIGIN. 009.3 DIARRHEA OF PRESUMED INFECTIOUS ORIGIN. 153.0 – 153.9 MALIGNANT NEOPLASM OF HEPATIC FLEXURE – …
What is the ICD 9 code for screening colonoscopy?
2012 ICD-9-CM Diagnosis Code V76.51. Special screening for malignant neoplasms of colon. Short description: Screen malig neop-colon. ICD-9-CM V76.51 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, V76.51 should only be used for claims with a date of service on or before September 30, 2015.
When is a screening colonoscopy becomes diagnostic?
Colorectal Cancer Screening ICD-9-CM diagnosis code for an average risk patient presenting for colonoscopy is: V76.51 Special Screening for Malignant Neoplasm, Colon Code V76.51 should be the first listed diagnosis code if the reason for the visit is specifically for the screening exam.
What are the Medicare guidelines for colonoscopy?
2012 ICD-9-CM Diagnosis Code V76.51 Special screening for malignant neoplasms of colon Short description: Screen malig neop-colon. ICD-9-CM V76.51 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, V76.51 should only be used for claims with a date of service on or before September 30, 2015.
.jpg)
What is the ICD 10 code for Encounter for colonoscopy?
Z12.11A screening colonoscopy should be reported with the following International Classification of Diseases, 10th edition (ICD-10) codes: Z12. 11: Encounter for screening for malignant neoplasm of the colon.May 1, 2016
How do you code a colonoscopy?
What's the right code to use for screening colonoscopy? For commercial and Medicaid patients, use CPT code 45378 (Colonoscopy, flexible, proximal to splenic flexure; diagnostic, with or without collection of specimen(s) by brushing or washing, with or without colon decompression [separate procedure]).
What is CPT code for screening colonoscopy?
Article GuidanceCOLORECTAL CANCER SCREENING GUIDELINESColorectal Cancer Screening Test/ProcedureCPT/HCPCS CodeScreening Fecal-Occult Blood Test82270 G0328Screening Flexible SigmoidoscopyG0104Screening Colonoscopy - individual at high riskG01055 more rows
Is a colonoscopy?
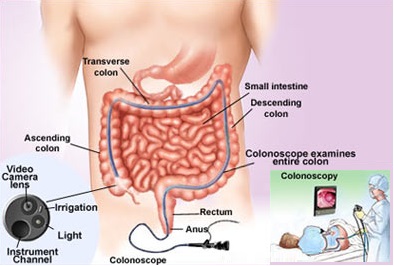
A colonoscopy (koe-lun-OS-kuh-pee) is an exam used to detect changes or abnormalities in the large intestine (colon) and rectum. During a colonoscopy, a long, flexible tube (colonoscope) is inserted into the rectum. A tiny video camera at the tip of the tube allows the doctor to view the inside of the entire colon.Apr 18, 2020
What is the ICD 10 code for incomplete colonoscopy?
Incomplete Colonoscopy B Incomplete Colonoscopies) are 44388, 45378, G0105, and G0121.Jul 8, 2021
What is diagnosis code Z86 010?
Personal history of colonic polypsTwo Sets of Procedure Codes Used for Screening Colonoscopy:Common colorectal screening diagnosis codesICD-10-CMDescriptionZ12.11Encounter for screening for malignant neoplasm of colonZ80.0Family history of malignant neoplasm of digestive organsZ86.010Personal history of colonic polypsDec 16, 2021
What does diagnosis code Z1211 mean?
Encounter for screening for malignant neoplasm of colonicd10 - Z1211: Encounter for screening for malignant neoplasm of colon.
What is the difference between modifier Pt and 33?
Modifier 33 is a valid CPT modifier and may be used for all payers. Check with individual payers for their instructions. Modifier PT is more specialized and will be used by fewer practices. It is a HCPCS modifier, used to indicate that a colorectal screening service converted to a diagnostic or therapeutic service.Apr 9, 2012
What is the code for colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code Z12.11 ( encounter for screening for malignant neoplasm of the colon ).
What is a colonoscopy screening?
As such, “screening” describes a colonoscopy that is routinely performed on an asymptomatic person for the purpose of testing for the presence of colorectal cancer or colorectal polyps. Whether a polyp or cancer is ultimately found does not ...
What are the global periods for colonoscopy?
Typically, procedure codes with 0, 10 or 90-day global periods include pre-work, intraoperative work, and post-operative work in the Relative Value Units (RVUs) assigned . As a result, CMS’ policy does not allow for payment of an Evaluation and Management (E/M) service prior to a screening colonoscopy. In 2005, the Medicare carrier in Rhode Island explained the policy this way:
Does Medicare cover colonoscopy?
However, diagnostic colonoscopy is a test performed as a result of an abnormal finding, sign or symptom. Medicare does not waive the co-pay and deductible when the intent of the visit is to perform a diagnostic colonoscopy. Medicare waives the deductible but not the co-pay when a procedure scheduled as a screening is converted to a diagnostic ...
Is E/M covered by Medicare?
Medicare defines an E/M prior to a screening colonoscopy as routine, and thus non-covered. However, when the intent of the visit is a diagnostic colonoscopy an E/M prior to the procedure ordered for a finding, sign or symptom is a covered service.
What does PT mean in CPT?
The PT modifier ( colorectal cancer screening test, converted to diagnostic test or other procedure) is appended to the CPT ® code.
Can you remove polyps at screening colonoscopy?
It is not uncommon to remove one or more polyps at the time of a screening colonoscopy. Because the procedure was initiated as a screening the screening diagnosis is primary and the polyp (s) is secondary. Additionally, the surgeon does not report the screening colonoscopy HCPCS code, but reports the appropriate code for the diagnostic or therapeutic procedure performed, CPT ® code 45379—45392.
General Information
CPT codes, descriptions and other data only are copyright 2020 American Medical Association. All Rights Reserved. Applicable FARS/HHSARS apply.
CMS National Coverage Policy
Title XVIII of the Social Security Act (SSA), §1862 (a) (1) (A) states that no Medicare payment shall be made for items or services that “are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.”
Article Guidance
The following billing and coding guidance is to be used with its associated Local Coverage Determination.#N#Coding Guidelines#N#Do not report a colonoscopy procedure code for an endoscopy performed with a sigmoidoscope on a patient with a normal length colon, even if the sigmoidoscope reaches proximal to the splenic flexure.
Bill Type Codes
Contractors may specify Bill Types to help providers identify those Bill Types typically used to report this service. Absence of a Bill Type does not guarantee that the article does not apply to that Bill Type.
Revenue Codes
Contractors may specify Revenue Codes to help providers identify those Revenue Codes typically used to report this service. In most instances Revenue Codes are purely advisory. Unless specified in the article, services reported under other Revenue Codes are equally subject to this coverage determination.
Popular Posts:
- 1. icd 9 code for copd without exacerbation
- 2. icd 10 code for thrombosed hemorrhoid
- 3. icd 10 code for great toe paronychia
- 4. the icd-10-cm code for right eye conjunctival granuloma is
- 5. icd 10 cm code for psychotic disorder
- 6. icd 10 cm code for tachycardia
- 7. icd 10 code for laceration lower lip
- 8. what is the icd 10 code for acute appendectomy
- 9. 2016 icd 10 code for chronic sarcoidosis
- 10. icd 10 code for osteomyelitis thoracic spine