V67.9
What is the ICD 9 code for follow up exam?
Unspecified follow-up examination. Short description: Follow-up exam NOS. ICD-9-CM V67.9 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, V67.9 should only be used for claims with a date of service on or before September 30, 2015.
Do you use a V or a DX code for follow up visits?
Follow up visits with resolved conditions are still coded with the same ICD-9 code as the first visit. See the link below. I use a V code and the the original Dx. So yes, both. I did not check the accuracy of your codes in particular, I just want to let you know that I use both a V and a Dx code.
How do you code a diagnosis that has been resolved?
If the diagnosis is resolved, you can't code it. You would report the appropriate V code for the follow-up (from the V67 category), then as a secondary code, you would report a V code for history of the condition that you are following up for. This is per the ICD-9-CM guidelines.
How do you code follow-up?
Follow-up visits, like initial visits, should be coded using the appropriate evaluation and management (E/M) code (i.e., 99211–99215). Given the limited interaction with the patient and limited work involved, the level of service is likely to be low (e.g., 99211 or 99212).
What is the ICD-10 code for a follow-up visit?
ICD-10 code Z09 for Encounter for follow-up examination after completed treatment for conditions other than malignant neoplasm is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What are ICD-9 procedure codes?
ICD-9-CM is the official system of assigning codes to diagnoses and procedures associated with hospital utilization in the United States. The ICD-9 was used to code and classify mortality data from death certificates until 1999, when use of ICD-10 for mortality coding started.
What is diagnosis code Z71 2?
Person consulting for explanation of examination or2022 ICD-10-CM Diagnosis Code Z71. 2: Person consulting for explanation of examination or test findings.
What is the ICD 10 code for aftercare?
Aftercare codes are found in categories Z42-Z49 and Z51. Aftercare is one of the 16 types of Z-codes covered in the 2012 ICD-10-CM Official Guidelines and Reporting.
What is the difference between follow up and aftercare?
Follow-up. The difference between aftercare and follow-up is the type of care the physician renders. Aftercare implies the physician is providing related treatment for the patient after a surgery or procedure. Follow-up, on the other hand, is surveillance of the patient to make sure all is going well.
What is an example of an ICD-9 code?
Most ICD-9 codes are three digits to the left of a decimal point and one or two digits to the right of one. For example: 250.0 is diabetes with no complications. 530.81 is gastroesophageal reflux disease (GERD).
What are ICD-9 10 and CPT codes?
ICD-10-CM diagnosis codes provide the reason for seeking health care; ICD-10-PCS procedure codes tell what inpatient treatment and services the patient got; CPT (HCPCS Level I) codes describe outpatient services and procedures; and providers generally use HCPCS (Level II) codes for equipment, drugs, and supplies for ...
Are ICD-9 codes still used in 2021?
CMS will continue to maintain the ICD-9 code website with the posted files. These are the codes providers (physicians, hospitals, etc.) and suppliers must use when submitting claims to Medicare for payment.
Can Z71 2 be primary diagnosis?
Z71.2 as principal diagnosis According to the tabular index, a symbol next to the code indicates that it is an unacceptable principal diagnosis per Medicare code edits. This applies for outpatient and inpatient care.
What is diagnosis code Z71 3?
Dietary counseling and surveillanceICD-10 code Z71. 3 for Dietary counseling and surveillance is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is diagnosis code Z712?
icd10 - Z712: Person consulting for explanation of examination or test findings.
What is Z09 code?
Z09 is a billable diagnosis code used to specify a medical diagnosis of encounter for follow-up examination after completed treatment for conditions other than malignant neoplasm.
What does "use additional code" mean?
Use Additional Code. Use Additional Code. The “use additional code” indicates that a secondary code could be used to further specify the patient’s condition. This note is not mandatory and is only used if enough information is available to assign an additional code.
Is Z09 a POA?
Z09 is exempt from POA reporting - The Present on Admission (POA) indicator is used for diagnosis codes included in claims involving inpatient admissions to general acute care hospitals. POA indicators must be reported to CMS on each claim to facilitate the grouping of diagnoses codes into the proper Diagnostic Related Groups (DRG). CMS publishes a listing of specific diagnosis codes that are exempt from the POA reporting requirement. Review other POA exempt codes here.
What is the code for inpatient consultation?
Inpatient consultations should be reported using the Initial Hospital Care code (99221-99223) for the initial evaluation, and a Subsequent Hospital Care code (99231-99233) for subsequent visits. Can you bill an office visit and hospital visit on the same day?
How long does it take to get a CPT code 99495?
CPT Code 99495 covers communication with the patient or caregiver within two business days of discharge. This can be done by phone, e-mail, or in person. It involves medical decision making of at least moderate complexity and a face-to-face visit within 14 days of discharge. The location of the visit is not specified.
What is CPT code 99211?
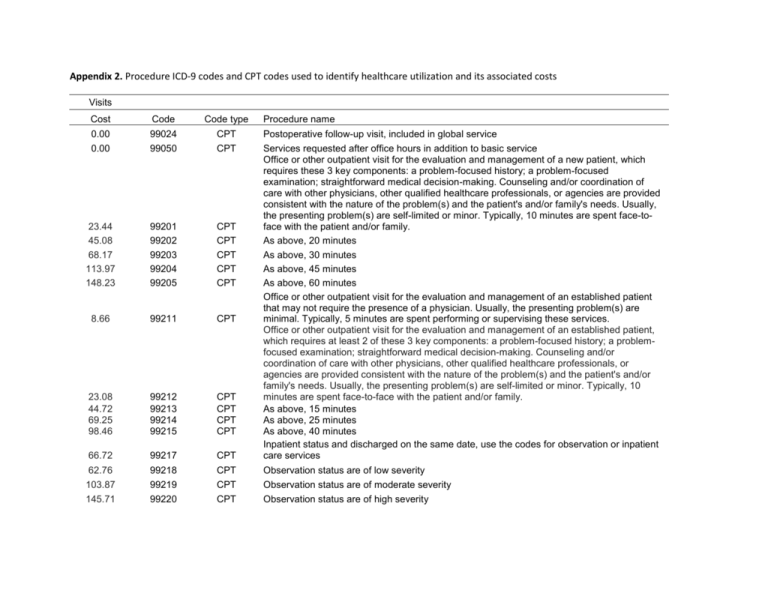
The CPT manual defines code 99211 as an office or other outpatient visit “that may not require the presence of a physician. Usually, the presenting problem(s) are minimal. Typically, five minutes are spent performing or supervising these services.”.
What is a modifier code?
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance.
Does Medicare accept 99241?
Medicare does not accept claims for either outpatient (99241-99245) or inpatient (99251-99255) consultations, and instead requires that services be billed with the most appropriate (non-consultation) E/M code. What is the CPT code for inpatient consultation? Inpatient consultations should be reported using the Initial Hospital Care code ...

Popular Posts:
- 1. icd 10 cm code for requesting sleeping pills
- 2. icd-10 code for fussiness in child 1 year old
- 3. icd 10 cm code for playing the drum
- 4. icd 10 code for right toe infection
- 5. what is the icd 10 code for hives
- 6. icd 9 code for stuttering
- 7. icd 10 code for bilateral hard of hearing
- 8. icd 10 code for incesible loss of urinating
- 9. icd 10 code for elevated alkaline phosphatase levels
- 10. icd 10 code for clinical sepsis