ICD-9 code 550.9 for Inguinal hernia without mention of obstruction or gangrene is a medical classification as listed by WHO under the range -HERNIA OF ABDOMINAL CAVITY (550-553).
Full
AnswerWhat is the ICD9 code for hernia?
ICD-9-CM (ICD-9, ICD9, ICD9CM) Diagnosis Codes - Group 55. 550.00 inguinal hernia gangrene unilateral nos ICD-9 Code; 550.01 inguinal hernia gangrene unilateral unspecified recurrent ICD-9 Code
What is the ICD 9 code for ventral hernia?
Short description: Ventral hernia NEC. ICD-9-CM 553.29 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, 553.29 should only be used for claims with a date of service on or before September 30, 2015.
What is the ICD code of hernia postoperative complication?
- T80 Complications following infusion, transfusion and therapeutic injection
- T81 Complications of procedures, not elsewhere classified
- T82 Complications of cardiac and vascular prosthetic devices, implants and grafts
- T83 Complications of genitourinary prosthetic devices, implants and grafts
What is the ICD 10 code for inguinal hernia incarcerated?
What is the ICD 10 code for inguinal hernia incarcerated? Hernia (K40-K46) Inguinal hernia (unilateral): · causing obstruction · incarcerated · irreducible · strangulated. } } } } K40.4. Unilateral or unspecified inguinal hernia, with gangrene. Inguinal hernia NOS with gangrene. K40.9.
What is the ICD 10 code for hernia?
ICD-10-CM Code for Unspecified abdominal hernia without obstruction or gangrene K46. 9.
What is the ICD 10 code for abdominal hernia?
Unspecified abdominal hernia without obstruction or gangrene K46. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM K46. 9 became effective on October 1, 2021.
What is the ICD 9 code for hernia repair?
53.953.9 Other hernia repair - ICD-9-CM Vol.
What is the ICD 10 code for left inguinal hernia?
ICD-10 Code for Inguinal hernia- K40- Codify by AAPC.
What is the ICD 10 code for history of hernia repair?
Other specified postprocedural states The 2022 edition of ICD-10-CM Z98. 89 became effective on October 1, 2021.
What is internal hernia?
Introduction. An internal hernia (IH) is defined as the protrusion of abdominal viscera, most commonly small bowel loops, through a peritoneal or mesenteric aperture into a compartment in the abdominal and pelvic cavity (1-3).
What is the code for right and left inguinal hernia?
3 Unilateral or unspecified inguinal hernia, with obstruction, without gangrene.
What is an indirect inguinal hernia?
Indirect inguinal hernias are the most common type of groin hernia. Indirect inguinal hernias occur when abdominal content such as fat or bowel pushes down along the inguinal canal. What is the inguinal canal? It is the tunnel through which a man's vas deferens and testicular vessels travel down into the scrotum.
What is a unilateral inguinal hernia?
An inguinal hernia occurs when tissue, such as part of the intestine, protrudes through a weak spot in the abdominal muscles. The resulting bulge can be painful, especially when you cough, bend over or lift a heavy object.
What is the root operation for hernia repair?
The two main root operations for hernia repair are Q-Repair, which is assigned when mesh is not used, and U-Supplement, which is assigned when mesh is used. Note that a code using root operation U-Supplement stands by itself as a hernia repair procedure and no additional code is required or assigned to capture the repair or use of mesh.
What is mesh for hernia repair?
For hernia repair without mesh, Z-No Device is used. For hernia repair with mesh, mesh is considered a device. There are three types of mesh: 1) Most mesh is made of synthetic materials such as polypropylene, polyester, and PTFE; 2) Some mesh is bioengineered from donated human tissue, such as from cadavers, and; 3) Some mesh is bioengineered from animal tissue such as bovine and porcine tissue (eg, PermacolTM Surgical Implant). Although there are three types of mesh, there are currently only two options for the device value. Synthetic meshes use J-Synthetic Substitute. Meshes made of either human and animal tissues currently use K-Nonautologous Tissue.5
What is the 49566?
49566 Repair recurrent incisional or ventral hernia; incarcerated or strangulated
Why is abdominal wall repair not coded separately?
Abdominal wall repair is not coded separately when an associated procedure is performed on an internal organ, because procedural steps necessary to close an operative site are considered integral.
Is abdominal wall repair the same as hernia repair?
In general, abdominal wall repair uses the same coding principles and the same code values as hernia repair. An abdominal wall repair is differentiated from a hernia repair by the ICD-10-CM diagnosis codes, not necessarily by the ICD-10-PCS procedure codes.
What is abdominal hernia?
A protrusion of abdominal structures through the retaining abdominal wall. It involves two parts: an opening in the abdominal wall, and a hernia sac consisting of peritoneum and abdominal contents. Abdominal hernias include groin hernia (hernia, femoral; hernia, inguinal) and ventral hernia.
What is a hernia with both gangrene and obstruction?
Hernia with both gangrene and obstruction is classified to hernia with gangrene. A protrusion of abdominal structures through the retaining abdominal wall. It involves two parts: an opening in the abdominal wall, and a hernia sac consisting of peritoneum and abdominal contents.
When will the ICD-10-CM K46.9 be released?
The 2022 edition of ICD-10-CM K46.9 became effective on October 1, 2021.
When was the last update in hernia coding?
The last update in hernia coding was in 2009.
What is abdominal hernia?
An abdominal hernia is a protrusion of part of the intestines through a weakened section of the abdominal cavity; herniations can occur in other parts of the body, such as muscle herniations. This article addresses abdominal hernias. Surgery is directed at permanently closing off the orifice through which the abdominal structures protrude.
What is the CPT code for mesh placement?
If you are new to general surgery coding, read on. Placement of mesh (49568) is an add-on code for incisional or ventral hernia repairs, performed via an open approach. The range of codes that CPT ® code 49568 may be reported with is 49560—49566.
What is CPT code 49659?
CPT ® code 49659, unlisted laparoscopy procedure, hernioplasty, herniorrhaphy, herniotomy is reported when a CPT ® code does not exist for the type of repair performed.
Is a hernia surgically reduced?
Surgery is directed at permanently closing off the orifice through which the abdominal structures protrude. Sometimes, the hernia can be manually reduced, but this is not a permanent intervention. There isn’t a code for medical reduction of a hernia, it is part of an E/M service.
Can you report a ventral hernia repair separately?
If either an incisional or ventral hernia repair is done at the time of another abdominal procedure, through the same incision, do not separately report the hernia repair. It is considered inclusive of the other procedure.
What are the codes for hernias?
Hernia codes (K40–K46) include acquired hernias, congenital hernias (except diaphragmatic or hiatus), and recurrent hernia.#N#Inguinal hernia K40-K40.91: This subcategory includes codes for direct inguinal, double inguinal, indirect, oblique inguinal, and scrotal hernias. To assign a code, you must know the location and laterality of the hernia, whether it’s with or without obstruction, whether it’s recurrent, and if there is gangrene present.#N#Femoral hernia K41.0-K41.91: This subcategory includes codes for paraumbilical hernias. To assign a code, you must know if the hernia is bilateral or unilateral, with or without obstruction, whether it’s recurrent, and if there is gangrene present.#N#Umbilical hernia K42-K42.9: To assign a code from this subcategory, you must know the hernia has an obstruction and/or gangrene present. An excludes 1 note with this category indicates that if an omphalocele (Q79.2 Exomphalos) is present, do not report these two codes together.#N#Ventral hernia K43.0-K43.9: To assign a code from this subcategory, know if the hernia is classified as an incisional hernia or a parastomal hernia, and if there is an obstruction and/or gangrene present.#N#Diaphragmatic hernia K44.0-K44.9: To assign a code from this subcategory, know if there is an obstruction and/or gangrene present. This code category includes hiatal hernia and esophageal or sliding hernia. There is an excludes 1 note that indicates not to report a congenital diaphragmatic hernia (Q79.0 Congenital diaphragmatic hernia) or a congenital hiatus hernia (Q40.1 Congenital hiatus hernia) at the same time as a code from this subcategory.#N#Other abdominal hernia K45-K45.8: This subcategory includes abdominal hernia, specified site, not elsewhere classified; lumbar hernia; obturator hernia; pudendal hernia; retroperitoneal hernia; and sciatic hernias. To assign a code, you must know if there is an obstruction and/or gangrene present.#N#Unspecified abdominal hernia K46-K46.9: Use a unspecified code only if documentation is imprecise and there is no way to query the reporting provider for more detail.
What is a hernia in medical terminology?
Hernia is a general term to describe a bulge or protrusion of an organ through the structure or muscle that usually contains it. Hernias can occur throughout the body (for instance, a herniated intervertebral disk), ...
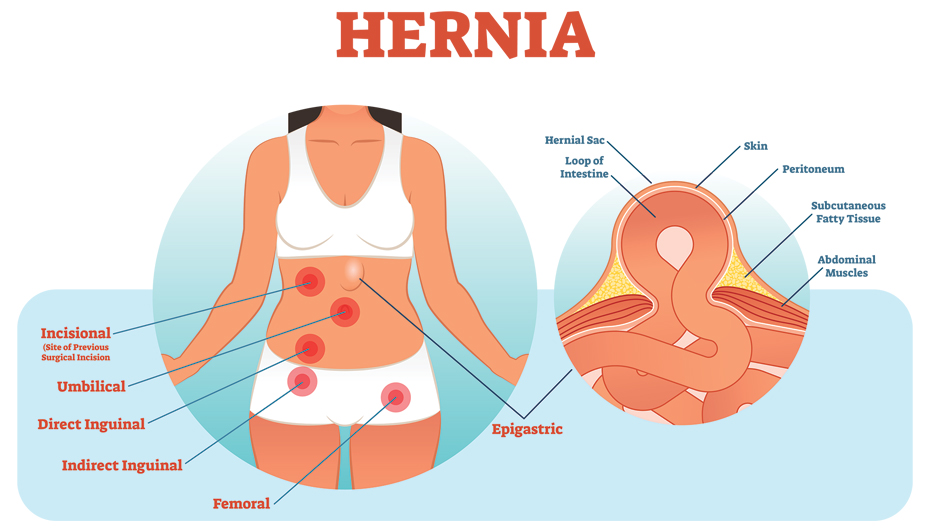
What are the different types of hernias?
Common hernia types include:#N#Inguinal: In this common form of hernia (75 percent of all hernias are of the inguinal variety), the intestine bulges through a weak area in the inguinal canal in the groin area. Inguinal her nias may be either direct (congenital) or indirect (acquired).#N#Femoral: These hernias occur in the area between the abdomen and the thigh, usually appearing as a bulge on the upper thigh.#N#Umbilical: The fascia of the navel is thinner than in the rest of the abdomen. An umbilical hernia occurs when contents protrude from the navel.#N#Ventral/Incisional: A defect in the abdominal wall at the site of a previous operative incision.#N#Diaphragmatic: A defect in the diaphragm (congenital or acquired) allows contents from the abdominal cavity to spill into the chest cavity.#N#Each of the above categories may include specific subcategories (e.g., femoral hernias include paraumbilical hernias). Additional hernia types include lumbar hernia, obturator hernia, pudendal hernia, and others.#N#2. Laterality#N#The concept of laterality only applies to inguinal and femoral hernias. For these hernia types, provider documentation must specify whether the hernia is bilateral or unilateral.#N#3. Complicated By#N#Complications of hernia include possible obstruction (documentation stating incarcerated, irreducible, or strangulated implies this) and the presence of gangrene.#N#If the provider can manually push the contents of the hernia sac (e.g., the intestine, in the case of an inguinal hernia) back through the fascial defect, the hernia is reducible. In some cases, the contents of the hernia sac become trapped in the opening caused by the fascial defect. Such incarcerated or strangulated hernias cannot be reduced and pose potential life-threatening danger.#N#A note at the beginning of the Hernia section in ICD-10-CM instructs that if a hernia has both obstruction and gangrene to classify it as having gangrene.#N#4. Temporal Parameters#N#Temporal parameters include status of recurrent and not specified as recurrent (e.g., Is this the first hernia at this location?).
How is a femoral hernia repaired?
The femoral hernia was repaired by suturing the iliopubic tract to Cooper’s ligament. K41.90 Unilateral femoral hernia, without obstruction or gangrene, not specified as recurrent. The femoral canal is the path through which the femoral artery, vein, and nerve leave the abdominal cavity to enter the thigh.
Why do umbilical hernias appear later in life?
If small, this type of hernia may close by age 2. Even if the area is closed at birth, umbilical hernias can appear later in life because this spot may remain a weaker place in the abdominal wall.
How do you know if you have a hernia?
Common symptoms of hernia vary, depending on the type. For asymptomatic hernia, the patient may have swelling or fullness at the hernia site. Although there’s little pain or tenderness, the patient may have an aching sensation that radiates into the area of the hernia.
Where do inguinal hernias occur?
Femoral: These hernias occur in the area between the abdomen and the thigh, usually appearing as a bul ge on the upper thigh. Umbilical: The fascia of the navel is thinner than in the rest of the abdomen.
Is abdominal wall repair the same as hernia repair?
In general, abdominal wall repair uses the same coding principles and the same code values as hernia repair. An abdominal wall repair is differentiated from a hernia repair by the ICD-10-CM diagnosis codes, not necessarily by the ICD-10-PCS procedure codes. Abdominal wall repair is not coded separately when an associated procedure is performed on an internal organ because procedural steps necessary to close an operative site are considered integral.1
Can a hernia be lysed?
Omental, intestinal, and other abdominal adhesions may be found and lysed during hernia repair, particularly for incarcerated hernias. Lysis is typically not coded separately because it is considered an integral procedural step necessary to reach the operative site. As an exception, lysis of adhesions can be coded separately when the surgeon clearly documents its clinical significance in the operative repair, for example, if the adhesions are extensive and require tedious lysis.
Popular Posts:
- 1. icd 10 code for left foot numbness
- 2. icd 10 code for injury to right elbow
- 3. icd 10 code for incidental finding on ct
- 4. icd 10 code for lumbar post laminectomy syndrome
- 5. icd 10 codes that support cpt code 93922 for 2018
- 6. 2015 icd 10 code for abnormal clavicle bone
- 7. icd 10 code for history of head trauma
- 8. icd 10 code for left arm tendonitis
- 9. icd 10 code medical clearance for jail
- 10. icd 10 code for fall off atv