| ICD-9-CM Procedure Code | Description |
|---|---|
| Discectomy | |
| 80.5 | Excision or destruction of intervertebral disc |
| 80.50 | Excision or destruction of intervertebral disc unspecified |
| 80.51 | Excision of intervertebral disc |
What diagnosis code is used for lumbar laminectomy?
Short description: Lumbar disc displacement. ICD-9-CM 722.10 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, 722.10 should only be used for claims with a date of service on or before September 30, 2015.
What is the ICD 10 code for lumbar disc herniation?
2015 ICD-9-CM Diagnosis Code V45.89. Other postprocedural status. 2015. Billable Thru Sept 30/2015. Non-Billable On/After Oct 1/2015. ICD-9-CM V45.89 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, V45.89 should only be used for claims with a date of service on or before September 30, 2015. For claims with a date of …
What is CPT code for lumbar decompression and fusion?
ICD-9/10: 722.1/ M51.16 Lumbar disc without myelopathy; sci-atica due to displacement of interver-tebral disc Suggested coding: 63042 Laminotomy (hemilaminec - tomy), with decompression of nerve roots(s); including partial facetectomy, foraminotomy and/or excision of herniated disc, reexploration, single in-terspace; Right lumbar L5-S1 63030-59 Laminotomy …
What would be appropriate ICD-10-CM code for lumbar stenosis?
Dec 12, 2019 · My understanding has always been, based on seasoned coders instructions, to report the anterior lumbar discectomy, with unlisted proc 64999, one time only, regardless of interspaces within the level. Another way it's reported is 63090, when the body of the report identifies either a retroperitoneal plane or transperitoneal, where the surgeon is going thru the …

What is the ICD 10 code for lumbar discectomy?
Other intervertebral disc displacement, lumbar region M51. 26 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM M51. 26 became effective on October 1, 2021.
How do you code a discectomy?
Discectomy is a single, standalone code, such as 63030 Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar.Dec 9, 2021
What is the ICD 10 code for status post discectomy?
2022 ICD-10-CM Diagnosis Code M96. 1: Postlaminectomy syndrome, not elsewhere classified.
What is the CPT code for lumbar discectomy?
Lumbar Decompression Procedures 63005 Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis.May 26, 2021
What discectomy means?
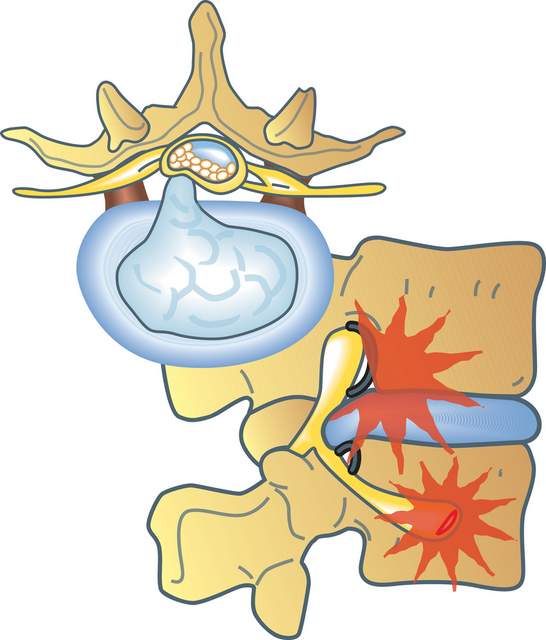
Discectomy is the surgical removal of part or all of a vertebral disc that has herniated. The disc is removed by first cutting the outer annulus fibrosis and removing the nucleus pulposus to relieve pressure on the nerve root.
Is a discectomy?
Discectomy literally means "cutting out the disc." A discectomy can be performed anywhere along the spine from the neck (cervical) to the low back (lumbar). The surgeon reaches the damaged disc from the back (posterior) of the spine—through the muscles and bone.
What is Postlaminectomy not elsewhere classified?
1 Postlaminectomy syndrome, not elsewhere classfied) is a term used to describe pain which persists in spite of back surgery attempted to relieve it and that it should only be coded when 'postlaminectomy syndrome' is documented.Jul 1, 2017
What is the ICD-10 code for status post back surgery?
Other specified postprocedural states The 2022 edition of ICD-10-CM Z98. 89 became effective on October 1, 2021.
What is the ICD-10 code for status post surgery?
ICD-10-CM Code for Encounter for surgical aftercare following surgery on specified body systems Z48. 81.
What is the difference between 63030 and 63042?
So 63042 is used for revision discectomies. And 63030, in addition to describing laminotomies performed with a discectomy to treat spinal disc herniation using an open procedure, can also describe those performed under endoscopic assistance.Jan 14, 2019
Does CPT code 63047 include discectomy?
When the laminectomy or laminotomy is performed primarily for spinal stenosis, the decompression procedure is the primary focus and if only a minor discectomy or no discectomy is performed in the procedure, then Codes 60345 or 63047 would be used.Jan 2, 2016
Is 63047 a bilateral procedure?
CPT® 63047 in section: Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single ... more.
What is a CT scan of the lumbar spine?
Radiologist’s report of a magnetic resonance image (MRI) or computerized tomography (CT) scan with myelogram of the lumbar spine within the past 12 months showing a lumbar spine abnormality. Report the selective nerve root injection results, if it is applicable to the patient’s diagnostic workup.
How long does back pain last?
The pain can vary from mild to disabling. Back pain is considered to be chronic if it lasts more than three months. Age-related disc degeneration, facet joint arthrosis and segmental instability are leading causes of chronic back pain.
What is decompression of the spine?
Decompression is the general term to describe removal of the spinal disk, bone, or tissue causing pressure and pain. Often, this is the only procedure performed. Examples include: laminectomy to decompress spinal canal and/or nerve roots (e.g., 63001-63017, 63045-+63048), discectomy to decompress spinal canal and/or nerve roots (e.g., 63020-+63035, 63040-+63044, 63055-+63057), corpectomy (e.g., 63081-+63091), fracture repair (e.g., 22325-+22328), etc.#N#CPT® designates the decompression codes as being per “vertebral segment” or per “interspace.” Decompression occurs at the interspace for discectomy codes (e.g., right L4-L5 interspace). Discectomy is a single, standalone code, such as 63030 Laminotomy (hemilaminectomy), with decompression of nerve root (s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar.#N#But decompression of the spinal canal can be coded per vertebral segment (63001-63017), or per level of foraminotomy (e.g., decompression of the L4 exiting nerve root via partial laminectomy at L4 and partial laminectomy at L5, with foraminotomy at L4-L5, is reported using one code: 63047 Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root [s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar).#N#Discern whether the approach was posterior or anterior to choose the correct code. Table A illustrates commonly used, standalone decompression codes for spine surgery.#N#Table A: Standalone decompression codes for spine surgery
Is spine coding difficult?
“It seems like coding spine cases is as complicated as doing the surgery,” said a spine surgeon at his first coding training session with me.#N#Spine procedure coding can make even the most confident coder squirm. But spine procedure coding doesn’t have to be difficult. In fact, it’s quite formulaic. Follow these five principles and spine procedure coding will go from scary to simple.
Do you need a bone graft code for fusion?
Because a fusion was performed, you must include a bone graft code. As with other graft codes in CPT®, the spinal bone graft codes are reported for harvesting the bone graft. The work of placing the bone graft is included in the arthrodesis/fusion codes. All spinal bone graft codes are add-on codes.
Does Medicare reimburse bone grafts?
Some payers (including Medicare) will incorrectly reimburse the instrumentation and some bone graft codes when billed with modifier 62; however, CPT® guidelines prohibit reporting the instrumentation and bone graft codes with modifier 62. Example 1.
Popular Posts:
- 1. icd 10 code for acute mucoid otitis media
- 2. icd 10 code for demetia
- 3. icd 10 code for tlif
- 4. icd 10 code for left knee medial and lateral meniscus tear
- 5. icd 10 code for avulsion fracture knee
- 6. icd 10 code for status post tpa
- 7. icd 10 code for axillary lymph node
- 8. icd 10 code for history of hypotension
- 9. icd 10 code for penile prosthesis
- 10. icd code for protime