Myasthenia gravis without (acute) exacerbation. G70.00 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2019 edition of ICD-10-CM G70.00 became effective on October 1, 2018.
ICD-9 Code 358.00 -Myasthenia gravis without (acute) exacerbation- Codify by AAPC.
Full
AnswerWhat is ICD 10 used for?
Used for medical claim reporting in all healthcare settings, ICD-10-CM is a standardized classification system of diagnosis codes that represent conditions and diseases, related health problems, abnormal findings, signs and symptoms, injuries, external causes of injuries and diseases, and social circumstances.
When did ICD 10 effective?
Work on ICD-10 began in 1983, became endorsed by the Forty-third World Health Assembly in 1990, and was first used by member states in 1994. It was replaced by ICD-11 on January 1, 2022.
What is the ICD 10 diagnosis code for?
The ICD-10-CM is a catalog of diagnosis codes used by medical professionals for medical coding and reporting in health care settings. The Centers for Medicare and Medicaid Services (CMS) maintain the catalog in the U.S. releasing yearly updates.
What is the prognosis with ocular myasthenia gravis?
The most common symptoms include:
- Tiring easily just from the act of chewing, especially chewy food such as meat
- Weak or droopy eyelids
- The weakness of the facial muscles causing a “snarling” smile
- Blurred or double vision
- Slurred or nasal speech
- Difficulty breathing, particularly when exercising or lying flat
- Difficulty with neck leading to difficulty in holding up the head
What is ocular MG?
What is MG in medical terms?
What is ptosis in MG?
What is the name of the disease that causes muscle fatigability and weakness?
What is the sensitivity of single fiber EMG?
What are the risk factors for MG?
Does sustained muscle activation affect NMJ?
See more
About this website
Cogan's lid twitch and eyelid hopping - Neurosigns
Cogan's lid twitch sign, characteristic of myasthenia gravis, consists of a brief overshoot twitch of lid retraction following sudden return of the eyes to primary position after a period of downgaze.(1-3) The lid will briefly twitch upwards then settle back to its previous position.
Treatment of ocular myasthenia gravis - PubMed
Myasthenia gravis (MG) is an autoimmune disorder that is characterized by variable weakness and fatigability. Often, MG presents with only ocular symptoms such as ptosis and diplopia. Treatment of ocular MG is aimed at relieving the symptoms of ptosis and diplopia, as well as preventing the developm …
Ocular myasthenia gravis: an update on diagnosis and treatment
OMG remains a primarily clinical diagnosis, but recent advances in laboratory testing can improve the diagnostic accuracy and should be used in appropriate clinical settings. The mainstay of treatment for OMG has not significantly changed over the past years, but the increasing availability of stero …
What are symptoms of Myasthenia Gravis (MG)?
Conquer Myasthenia Gravis 275 N. York Street, Suite 201 Elmhurst, IL 60126. [email protected] (800) 888-6208
What is ocular MG?
Ocular MG affects only the ocular muscles. Systemic MG affects the ocular muscles (often the presenting sign) and other voluntary muscles. Approximately 85% of patients presenting with only ocular signs and symptoms of MG will develop systemic MG within 2 years of presentation.
What is MG in medical terms?
Myasthenia Gravis (MG) is an autoimmune disease in which antibodies destroy neuromuscular connections resulting in muscle weakness and fatigability. MG affects voluntary muscles of the body, but the muscles and motor nerves are intact. Smaller muscles tend to be affected first, larger muscles become affected as the disease progresses.
What is ptosis in MG?
Since ptosis is the most common presenting symptom in MG, it is important to go through its differential diagnosis. Ptosis is defined as margin to reflex diameter 1 (MRD 1) of less than 2mm or an asymmetry of more than 2mm between eyes. Normal palpebral fissure (PF) vertical length is about 9mm, a ptotic lid has a PF < 9mm. Myasthenia gravis with ptosis has an extensive differential diagnosis. This includes: an intracranial lesion, tumor, pituitary adenoma, aneurysm, fascicular lesion of CN 3, evolving CN 3 palsy, post-viral neuropathy, thyroid disorders *, migraines, meningitis, Horner's syndrome, levator aponeurosis, chronic progressive external ophthalmoplegia (CPEO), and developmental myopathy of the levator palpebrae superioris muscle.
What is the name of the disease that causes muscle fatigability and weakness?
Myasthenia Gravis. Myasthenia Gravis is an autoimmune disease which results in muscle fatigability and weakness throughout the day. Symptoms improve with rest. Its main symptoms, which the ophthalmologist may encounter, are ptosis, diplopia, variable extra-ocular muscle palsies or incomitant strabismus, and external ophthalmoplegia.
What is the sensitivity of single fiber EMG?
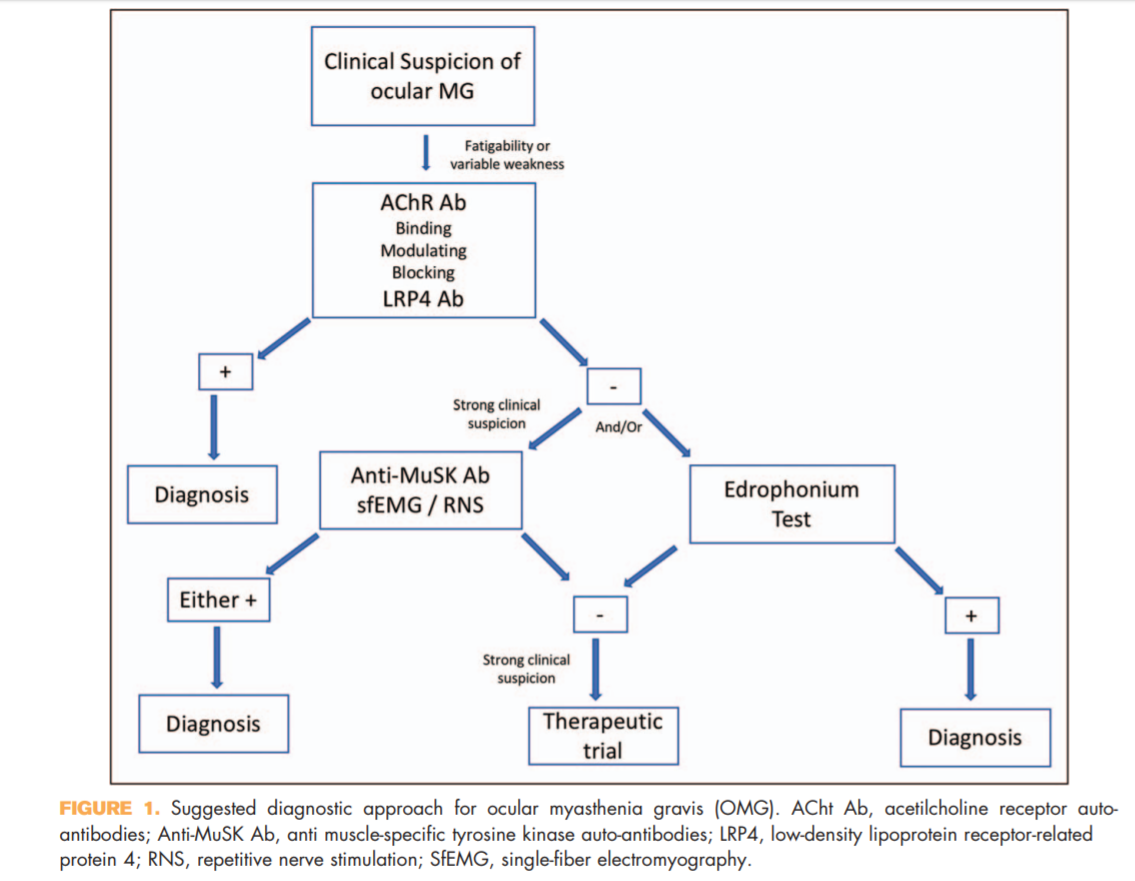
The single fiber EMG is highly sensitive for ocular myasthenia, with a sensitivity of 88-99%. This is a good diagnostic test for congenital myasthenia gravis.
What are the risk factors for MG?
There are no known risk factors for acquired MG. Aggravating factors, such as pregnancy, emotional stress, infections, excessive alcohol, UV light, extreme temperatures, thyroid disease and certain medications may worsen the disease and have been linked to myasthenic crises.
Does sustained muscle activation affect NMJ?
Normally, with sustained muscle activation, smaller amounts of ACh are released with each successive impulse, but transmission is not affected and muscular strength is maintained. In MG, the reduced amount of ACh released with sustained muscle activation results in further impairment of the NMJ transmission. This is the basis of muscle fatigability and the electrophysiologic decrement seen in MG.
Is striated muscle a thymoma?
Antibodies to striated muscle have also been noted in MG. They are elevated in 30% of adult MG patients and are associated with thymoma, and they are positive in 80% of thymomatous MG Thymoma occurs in 5%–20% of patients with generalized MG, but it is rare in OM patients.
Can ocular myasthenia be diagnosed?
Patients with ocular myasthenia often have negative serum tests for acetylcholine receptor antibodies, and recently published studies confirm that several office-based tests can aid in the diagnosis of ocular myasthenia in particular. Knowledge of the electrophysiologic tests available will also expand the clinician’s armamentarium. Since no one perfect diagnostic or clinical test exists for ocular myasthenia (OM), it is critical to understand the advantages and limitations of all the diagnostic techniques available.
Is there a perfect test for ocular myasthenia?
Since no one perfect diagnostic or clinical test exists for ocular myasthenia (OM), it is critical to understand the advantages and limitations of all the diagnostic techniques available.
Can ocular myasthenia be diagnosed with acetylcholine?
Patients with ocular myasthenia often have negative serum tests for acetylcholine receptor antibodies, and recently published studies confirm that several office-based tests can aid in the diagnosis of ocular myasthenia in particular. Knowledge of the electrophysiologic tests available will also expand the clinician’s armamentarium.
What is ocular myasthenia gravis?
What is ocular myasthenia gravis? Ocular myasthenia gravis is a form of myasthenia gravis (MG) in which the muscles that move the eyes and control the eyelids are easily fatigued and...
How do you know if you have MG?
Problems with double vision and drooping eyelids are often the first symptoms of MG. Although most people have eye problems at the onset of MG, they may have other muscle weakness or develop other muscle weakness in the first two years after MG symptoms begin. About 15% of people with MG will have only ocular problems (ocular MG). If weakness of other muscles develops over time, the MG changes from ocular MG to generalized MG. About half of all people with ocular issues related to MG in the first year will develop generalized MG. People that have had only ocular MG symptoms for five years or more will most likely not develop generalized MG.
Can you have eyelid surgery with MG?
Eyelid or eye muscle surgery is generally not recommended for people with MG
Can MG cause eye muscle weakness?
One hypothesis is that people with MG may simply notice eye weakness more often than mild weakness in other muscle groups in the body. Another hypothesis is that the eye and eyelid muscles are structurally different from muscles in the trunk and limbs. For example, these parts of the body have fewer acetylcholine (AChR) receptors, which is where the defect occurs in autoimmune MG. Eye muscles contract much more rapidly than other muscles and may be more likely to fatigue.
Can ocular MG cause weakness?
People with ocular MG do not have difficulty swallowing, speaking or breathing, nor do they have weakness of the arms or legs. Descriptions of the symptoms that people with ocular MG may have include:
What is myasthenia gravis?
Myasthenia gravis, ocular. Ocular myasthenia. Clinical Information. A chronic autoimmune neuromuscular disorder characterized by skeletal muscle weakness. It is caused by the blockage of the acetylcholine receptors at the neuromuscular junction.
How does myasthenia gravis affect the body?
Myasthenia gravis is disease that causes weakness in the muscles under your control. It happens because of a problem in communication between your nerves and muscles. Myasthenia gravis is an autoimmune disease. Your body's own immune system makes antibodies that block or change some of the nerve signals to your muscles. This makes your muscles weaker.common symptoms are trouble with eye and eyelid movement, facial expression and swallowing. But it can also affect other muscles. The weakness gets worse with activity, and better with rest..there are medicines to help improve nerve-to-muscle messages and make muscles stronger. With treatment, the muscle weakness often gets much better. Other drugs keep your body from making so many abnormal antibodies. There are also treatments which filter abnormal antibodies from the blood or add healthy antibodies from donated blood. Sometimes surgery to take out the thymus gland helps.for some people, myasthenia gravis can go into remission and they do not need medicines. The remission can be temporary or permanent.if you have myasthenia gravis, it is important to follow your treatment plan. If you do, you can expect your life to be normal or close to it.
What is the term for a disease that causes weakness in the muscles under your control?
Disease characterized by progressive weakness and exhaustibility of voluntary muscles without atrophy or sensory disturbance and caused by an autoimmune attack on acetylcholine receptors at the neuromuscular junction. Myasthenia gravis is disease that causes weakness in the muscles under your control.
When will the ICD-10 G70.00 be released?
The 2022 edition of ICD-10-CM G70.00 became effective on October 1, 2021.
Can myasthenia gravis go into remission?
The remission can be temporary or permanent.if you have myasthenia gravis, it is important to follow your treatment plan.
How does ocular myasthenia gravis affect the eye?
So, ocular myasthenia gravis affects the muscles that move the eyes and eyelids. The most common symptoms of ocular MG are: 1,3. Double vision (seeing 2 objects where there is 1) and trouble focusing occur because the muscles that keep the eyes aligned become weak.
What is the best treatment for ocular myasthenia gravis?
Treatment. An acetylcholinesterase inhibitor may be the only drug needed to control mild to moderate ocular myasthenia gravis. Steroids or another immunosuppressant drug may be added if symptoms are not controlled or flares become frequent or serious.
What is the most common antibody for MG?
Only half of people with ocular MG test positive for the antibodies that cause MG. People with no detectable antibodies are referred to as seronegative. For those that do have detectable antibodies, AChR (acetylcholine receptor) antibodies are the most common. LRP4 antibodies are the next most common. 2
What is MG in 2021?
Ocular MG is much less common, affecting only 15 percent of people with myasthenia gravis. 1-2. Ocular means “of the eye or vision.”. So, ocular myasthenia gravis affects the muscles that move the eyes and eyelids. The most common symptoms of ocular MG are: 1,3.
What is refractory myasthenia gravis?
If someone’s myasthenia gravis does not respond well to treatment, it may be called refractory MG. Only 15 percent of people with MG have refractory myasthenia gravis. 6
Does prednisolone help with myasthenia gravis?
Some studies seem to suggest that prednisolone treatment (a steroid) reduces the risk of ocular MG progressing to generalized MG. However, this has not been confirmed. 2. If someone’s myasthenia gravis does not respond well to treatment, it may be called refractory MG. Only 15 percent of people with MG have refractory myasthenia gravis. 6.
Can MG cause weakness in the face?
While droopy eyelids and double vision are common early signs of all forms of myasthenia gravis, people with ocular MG never go on to develop muscle weakness in their face, neck, arms, or legs.
What is ocular MG?
Ocular MG affects only the ocular muscles. Systemic MG affects the ocular muscles (often the presenting sign) and other voluntary muscles. Approximately 85% of patients presenting with only ocular signs and symptoms of MG will develop systemic MG within 2 years of presentation.
What is MG in medical terms?
Myasthenia Gravis (MG) is an autoimmune disease in which antibodies destroy neuromuscular connections resulting in muscle weakness and fatigability. MG affects voluntary muscles of the body, but the muscles and motor nerves are intact. Smaller muscles tend to be affected first, larger muscles become affected as the disease progresses.
What is ptosis in MG?
Since ptosis is the most common presenting symptom in MG, it is important to go through its differential diagnosis. Ptosis is defined as margin to reflex diameter 1 (MRD 1) of less than 2mm or an asymmetry of more than 2mm between eyes. Normal palpebral fissure (PF) vertical length is about 9mm, a ptotic lid has a PF < 9mm. Myasthenia gravis with ptosis has an extensive differential diagnosis. This includes: an intracranial lesion, tumor, pituitary adenoma, aneurysm, fascicular lesion of CN 3, evolving CN 3 palsy, post-viral neuropathy, thyroid disorders *, migraines, meningitis, Horner's syndrome, levator aponeurosis, chronic progressive external ophthalmoplegia (CPEO), and developmental myopathy of the levator palpebrae superioris muscle.
What is the name of the disease that causes muscle fatigability and weakness?
Myasthenia Gravis. Myasthenia Gravis is an autoimmune disease which results in muscle fatigability and weakness throughout the day. Symptoms improve with rest. Its main symptoms, which the ophthalmologist may encounter, are ptosis, diplopia, variable extra-ocular muscle palsies or incomitant strabismus, and external ophthalmoplegia.
What is the sensitivity of single fiber EMG?
The single fiber EMG is highly sensitive for ocular myasthenia, with a sensitivity of 88-99%. This is a good diagnostic test for congenital myasthenia gravis.
What are the risk factors for MG?
There are no known risk factors for acquired MG. Aggravating factors, such as pregnancy, emotional stress, infections, excessive alcohol, UV light, extreme temperatures, thyroid disease and certain medications may worsen the disease and have been linked to myasthenic crises.
Does sustained muscle activation affect NMJ?
Normally, with sustained muscle activation, smaller amounts of ACh are released with each successive impulse, but transmission is not affected and muscular strength is maintained. In MG, the reduced amount of ACh released with sustained muscle activation results in further impairment of the NMJ transmission. This is the basis of muscle fatigability and the electrophysiologic decrement seen in MG.
Popular Posts:
- 1. icd 10 code for advance directive counseling
- 2. icd 9 code for ulcer foot
- 3. icd 10 cm code for left breast cancer
- 4. icd 10 cm code for left wrist sprain
- 5. correct icd-10-cm code for right upper lid blepharochalasis is
- 6. icd 10 code for polycarbonate
- 7. icd 10 code for salmonellosis
- 8. icd-10 code for osteochondral defect medial femoral condyle right knee
- 9. icd 9 code for numbness in fingers
- 10. icd-10 code for wound