ICD-9-CM Diagnosis Code 157.9 : Malignant neoplasm of pancreas, part unspecified.
What is the diagnosis code for pancreatic cancer?
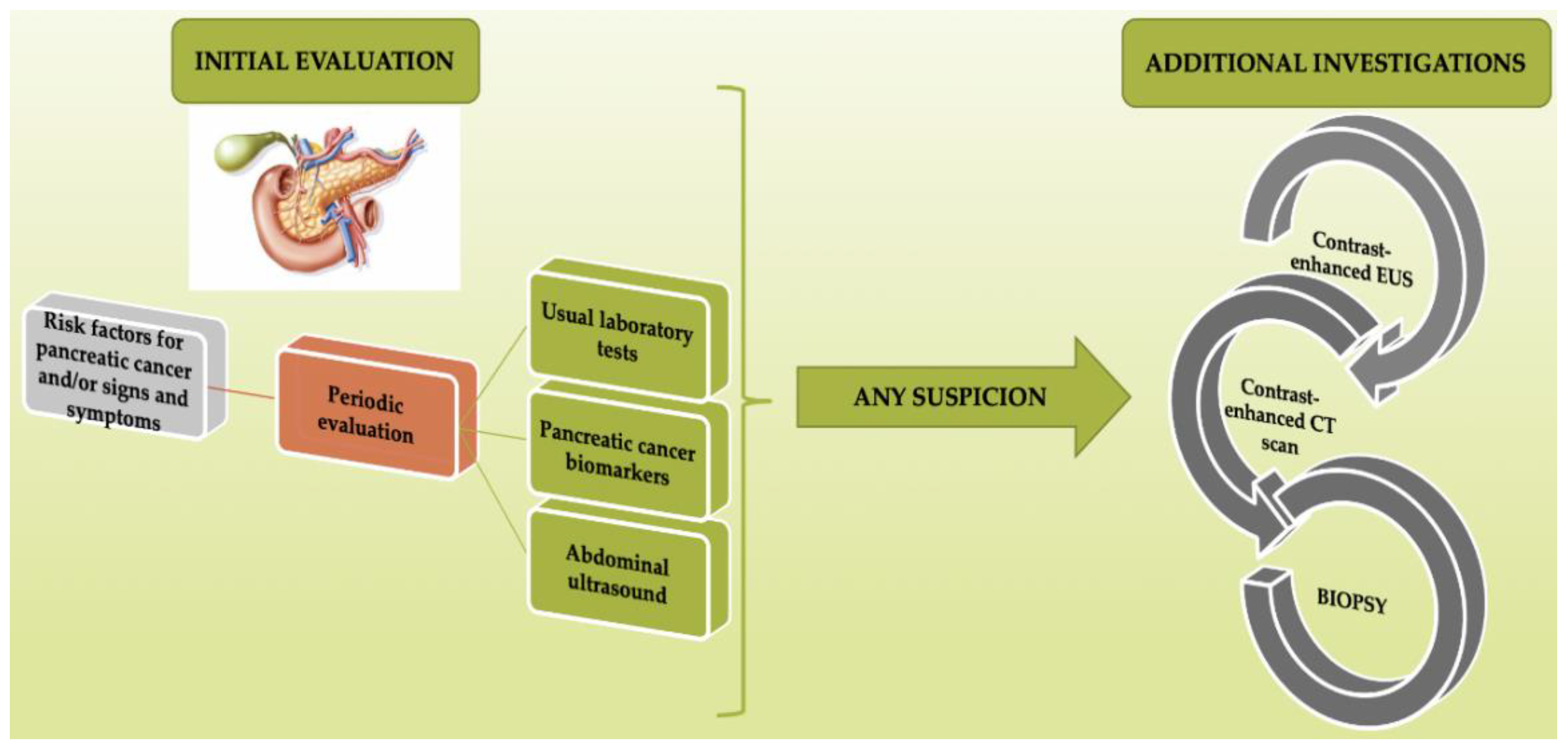
- CT scan (88.01);
- MRI (88.87); • endoscopic retrograde cholangiopancreatiogaphy (51.10); • endoscopic ultrasound (88.74 and a code for the endoscopy—code assignment will depend on location) • percutaneous transhepatic cholangiography (87.51); • biopsy of ...
- Respectable — all tumor nodules can be removed.
What is the ICD 9 code for history of cancer?
- accessory sinus V10.22
- adrenal V10.88
- anus V10.06
- bile duct V10.09
- bladder V10.51
- bone V10.81
- brain V10.85
- breast V10.3
- bronchus V10.11
- cervix uteri V10.41
What is the ICD - 9 code for chronic pancreatitis?
ICD-9 Code 577.1 Chronic pancreatitis. ICD-9 Index; Chapter: 520–579; Section: 570-579; Block: 577 Diseases of pancreas; 577.1 - Chronic pancreatitis
What is the ICD - 9 code for pancreatic lesion?
- Atrophy, atrophic pancreas (duct) (senile) 577.8
- Burke's syndrome 577.8
- Calcification pancreas 577.8
- Calculus, calculi, calculous 592.9 pancreas (duct) 577.8
- Cirrhosis, cirrhotic 571.5 pancreas (duct) 577.8
- Clarke-Hadfield syndrome (pancreatic infantilism) 577.8
- Colic (recurrent) 789.7 pancreas 577.8
- Congestion, congestive pancreas 577.8
What is the ICD 9 code for pancreatic cancer?
C25. 9 converts to ICD-9-CM: 157.9 - Malignant neoplasm of pancreas, part unspecified.
What is the ICD-10-CM code for primary pancreatic cancer?
Malignant neoplasm of pancreas, unspecified C25. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM C25. 9 became effective on October 1, 2021.
Is pancreatic cancer primary or secondary?
The majority of pancreatic tumors are primary. The pancreas can however be the site of metastasis from renal cell cancer, lung, colon and breast cancers.
What is the most common primary pancreatic malignancy?
Also called ductal carcinoma, adenocarcinoma, is the most common type of pancreatic cancer, accounting for more than 90 percent of pancreatic cancer diagnoses. This cancer occurs in the lining of the ducts in the pancreas. It's also possible for adenocarcinoma to develop from the cells that create pancreatic enzymes.
What is ICD-10 C25?
2022 ICD-10-CM Diagnosis Code C25: Malignant neoplasm of pancreas.
What is the ICD-10 code for stage IV pancreatic cancer?
C25. 4 - Malignant neoplasm of endocrine pancreas | ICD-10-CM.
Are there 2 types of pancreatic cancer?
Pancreatic tumors are either exocrine or neuroendocrine (endocrine) tumors. This is based on the type of cell they start in. Knowing the type of tumor is important because each type acts differently and responds to different treatments. Within these types, each tumor's biology is different.
Is pancreatic cancer a secondary cancer?
This is called a second cancer. Unfortunately, being treated for pancreatic cancer doesn't mean you can't get another cancer. People who have had pancreatic cancer can still get the same types of cancers that other people get. In fact, they might be at higher risk for certain types of cancer.
What type of cancer is pancreatic cancer?
Exocrine cancers are by far the most common type of pancreas cancer. If you are told you have pancreatic cancer, it's most likely an exocrine pancreatic cancer. Pancreatic adenocarcinoma: About 95% of cancers of the exocrine pancreas are adenocarcinomas. These cancers usually start in the ducts of the pancreas.
Where are most pancreatic cancers located?
Approximately 65% of pancreatic cancers occur in the head (HD) of the pancreas, whereas 15% occur in the body and tail (BT); the remaining lesions diffusely involve the gland 13.
What is the difference between adenocarcinoma and neuroendocrine?
While each type of tumor can spread (metastasize) from the pancreas to other organs, pancreatic neuroendocrine tumors usually spread over a period of years. Pancreatic adenocarcinoma, on the other hand, typically spreads over a period of months.
Are most pancreatic tumors malignant?
There are two types of tumors that grow in the pancreas: exocrine or neuroendocrine tumors. About 93% of all pancreatic tumors are exocrine tumors, and the most common kind of pancreatic cancer is called adenocarcinoma. Pancreatic adenocarcinoma is what people usually mean when they say they have pancreatic cancer.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is the pancreas?
The pancreas is a gland behind your stomach and in front of your spine. It produces juices that help break down food and hormones that help control blood sugar levels. Cancer of the pancreas is the fourth-leading cause of cancer death in the United States Some risk factors for developing pancreatic cancer include.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What chapter is functional activity?
Functional activity. All neoplasms are classified in this chapter, whether they are functionally active or not. An additional code from Chapter 4 may be used, to identify functional activity associated with any neoplasm. Morphology [Histology]
Can multiple neoplasms be coded?
For multiple neoplasms of the same site that are not contiguous, such as tumors in different quadrants of the same breast, codes for each site should be assigned. Malignant neoplasm of ectopic tissue. Malignant neoplasms of ectopic tissue are to be coded to the site mentioned, e.g., ectopic pancreatic malignant neoplasms are coded to pancreas, ...
What is the code for metastatic cancer?
If the documentation states the cancer is a metastatic cancer, but does not state the site of the metastasis, the coder will assign a code for the primary cancer, followed by code C79.9 secondary malignant neoplasm of unspecified site.
What is the code for primary cancer?
If the site of the primary cancer is not documented, the coder will assign a code for the metastasis first, followed by C80.1 malignant (primary) neoplasm, unspecified. For example, if the patient was being treated for metastatic bone cancer, but the primary malignancy site is not documented, assign C79.51, C80.1.
When coding malignant neoplasms, there are several coding guidelines we must follow?
When coding malignant neoplasms, there are several coding guidelines we must follow:#N#To properly code a malign ant neoplasm, the coder must first determine from the documentation if the neoplasm is a primary malignancy or a metastatic (secondary) malignancy stemming from a primary cancer.
What is C50.xx?
For instance, a patient who has primary breast cancer (C50.xx) who is now seen for metastatic bone cancer will have a code for the secondary bone cancer (C79.51) sequenced before a code for the primary breast cancer (C50.xx). When a current cancer is no longer receiving treatment of any kind, it is coded as a history code.
What is a history code for cancer?
When a current cancer is no longer receiving treatment of any kind, it is coded as a history code. For instance, the patient had breast cancer (C50.xx) and underwent a mastectomy, followed by chemoradiation. The provider documents that the patient has no evidence of disease (NED).
What is the Z85 code for a primary malignancy?
When a primary malignancy has been previously excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy at that site, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy. Any mention of extension, invasion, or metastasis to another site is coded as a secondary malignant neoplasm to that site. The secondary site may be the principal or first-listed with the Z85 code used as a secondary code.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion '), unless the combination is specifically indexed elsewhere. For multiple neoplasms of the same site that are not contiguous such as tumors in different quadrants of the same breast, codes for each site should be assigned.
What is Chapter 2 of the ICD-10-CM?
Chapter 2 of the ICD-10-CM contains the codes for most benign and all malignant neoplasms. Certain benign neoplasms , such as prostatic adenomas, may be found in the specific body system chapters. To properly code a neoplasm, it is necessary to determine from the record if the neoplasm is benign, in-situ, malignant, or of uncertain histologic behavior. If malignant, any secondary ( metastatic) sites should also be determined.
What is C80.0 code?
Code C80.0, Disseminated malignant neoplasm, unspecified, is for use only in those cases where the patient has advanced metastatic disease and no known primary or secondary sites are specified. It should not be used in place of assigning codes for the primary site and all known secondary sites.
When a pregnant woman has a malignant neoplasm, should a code from subcatego
When a pregnant woman has a malignant neoplasm, a code from subcategory O9A.1 -, malignant neoplasm complicating pregnancy, childbirth, and the puerperium, should be sequenced first, followed by the appropriate code from Chapter 2 to indicate the type of neoplasm. Encounter for complication associated with a neoplasm.
What is the code for leukemia?
There are also codes Z85.6, Personal history of leukemia, and Z85.79, Personal history of other malignant neoplasms of lymphoid, hematopoietic and related tissues. If the documentation is unclear as to whether the leukemia has achieved remission, the provider should be queried.
What is C80.1?
Code C80.1, Malignant ( primary) neoplasm, unspecified, equates to Cancer, unspecified. This code should only be used when no determination can be made as to the primary site of a malignancy. This code should rarely be used in the inpatient setting.
Popular Posts:
- 1. icd 10 code for ruptured ovarian cyst unspecified side
- 2. 2019 icd 10 code for right leg cellulitis
- 3. icd 9 code for labial ulcer
- 4. icd 10 code for osteoarthritis right leg
- 5. icd 10 cm code for rheumatoid arthritis
- 6. icd 10 code for infectious disease
- 7. icd 10 code for slow feeding in newborn
- 8. icd 10 code for rhinorhea
- 9. icd 10 code for e87.6
- 10. 2019 icd 10 code for twisted ankle