What's the right ICD-9 code to use for screening colonoscopy? Common diagnosis codes for colorectal cancer screening include: V76. 51 (Special screening for malignant neoplasms of colon).
How do you code a screening colonoscopy?
Special screening for malignant neoplasms of colon Short description: Screen malig neop-colon. ICD-9-CM V76.51 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, V76.51 should only be used for claims with a date of service on or before September 30, 2015.
What is the ICD - 9 code for screening?
4 rows · · Two Sets of Procedure Codes Used for Screening Colonoscopy: CPT ® code 45378. Colonoscopy, ...
How to code screening and diagnostic colonoscopy?
· ICD-9 Codes that Support Medical Necessity for colonoscopy procedures Lori January 26, 2012 Colonscopy CPT codes 2 Comments 009.0 – 009.1 INFECTIOUS COLITIS …
What is the diagnosis code for screening colonoscopy?
Procedure code: G0121 ( Average risk screening) or 45378-33 ( Diagnostic colonoscopy with modifier 33 indicating this is a preventive service ). Diagnosis code: V76.51 ( Special screening …
What is the ICD code for screening colonoscopy?
A screening colonoscopy should be reported with the following International Classification of Diseases, 10th edition (ICD-10) codes: Z12. 11: Encounter for screening for malignant neoplasm of the colon.
What is the ICD-10 code for colon screening?
ICD-10 code Z12. 11 for Encounter for screening for malignant neoplasm of colon is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
How do I code a Medicare screening colonoscopy?
45380 – Colonoscopy, flexible; with biopsy, single or multiple.45381 – Colonoscopy, flexible; with directed submucosal injection(s), any substance.45382 – Colonoscopy, flexible; with control of bleeding, any method.More items...
What is the difference between a screening and a diagnostic colonoscopy?
A screening colonoscopy will have no out-of-pocket costs for patients (such as co-pays or deductibles). A “diagnostic” colonoscopy is a colonoscopy that is done to investigate abnormal symptoms, tests, prior conditions or family history.
Do you use Z12 11 on surveillance colonoscopy?
There are 2 different sets of screening colonoscopy codes: There are payors that accept the Z12. 11 (encounter for screening for malignant neoplasm of colon) in the first coding position, while other payors either require this diagnosis in a subsequent position behind family history codes or prefer to see the Z12.
What is the difference between 45378 and 45380?
A family of CPT codes applies to colonoscopy. For example, code 45378 applies to a colonoscopy in which no polyp is detected, while codes 45380-45385 apply to colonoscopy that involves an intervention (e.g., 45385 is the code for colonoscopy with polypectomy.)
What is screening colonoscopy?
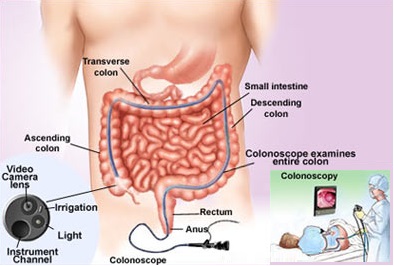
Colonoscopy. This is similar to flexible sigmoidoscopy, except the doctor uses a longer, thin, flexible, lighted tube to check for polyps or cancer inside the rectum and the entire colon. During the test, the doctor can find and remove most polyps and some cancers.
How do I bill for a patient seen in our office prior to a screening colonoscopy with no GI symptoms and who is otherwise healthy?
How do I bill for a patient seen in our office prior to a screening colonoscopy with no GI symptoms and who is otherwise healthy? A visit prior to a screening colonoscopy for a healthy patient is not billable.
Does Medicare pay for diagnostic colonoscopy?
Colonoscopies. Medicare covers screening colonoscopies once every 24 months if you're at high risk for colorectal cancer. If you aren't at high risk, Medicare covers the test once every 120 months, or 48 months after a previous flexible sigmoidoscopy.
Is a screening colonoscopy considered preventive care?
A colonoscopy is an important preventive care screening test that helps detect pre-cancer or colon cancer. The earlier signs of colon cancer are detected, the easier it is to prevent or treat the disease.
Are there two types of colonoscopy?
There are two types of colonoscopy: screening and diagnostic. Talk to you doctor about which you may need and understand your benefits for both types before the procedure.
Is Z12 11 a preventive code?
The colonoscopy or sigmoidoscopy is still classified as a preventive service eligible for coverage at the no-member-cost-share benefit level. a. Submit the claim with Z12. 11 (Encounter for screening for malignant neoplasm of colon) as the first-listed diagnosis code; this is the reason for the service or encounter.
What does Z12 11 mean?
Encounter for screening for malignant neoplasm of colon Z12. 11 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
Does Medicare cover S0285?
Consistent with Medicare guidelines, code S0285 will not be reimbursed separately for Medicare product lines. If you have any questions with respect to this notice, please contact your Professional Relations Representative.
What is CPT G0104?
HCPCS code G0104 for Colorectal cancer screening; flexible sigmoidoscopy as maintained by CMS falls under Screening Examinations and Disease Management Training .
What is the code for colonoscopy?
To report screening colonoscopy on a patient not considered high risk for colorectal cancer, use HCPCS code G0121 and diagnosis code Z12.11 ( encounter for screening for malignant neoplasm of the colon ).
What is a colonoscopy screening?
As such, “screening” describes a colonoscopy that is routinely performed on an asymptomatic person for the purpose of testing for the presence of colorectal cancer or colorectal polyps. Whether a polyp or cancer is ultimately found does not ...
What does modifier PT mean in CPT?
Add modifier PT to the CPT ® codes above to indicate that a scheduled screening colonoscopy was converted to diagnostic or therapeutic. Modifier PT should be added to the anesthesia service as well. This informs Medicare that it was a service performed for screening and the patient will not be charged a deductible. There will be a co-pay due.
What is G0121 in medical terms?
G0121 ( colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk.
How often can you get a colonoscopy with Medicare?
Medicare beneficiaries without high risk factors are eligible for screening colonoscopy every ten years. Beneficiaries at high risk for developing colorectal cancer are eligible once every 24 months. Medicare considers an individual at high risk for developing colorectal cancer as one who has one or more of the following:
What is a G0121?
Colonoscopy, flexible, proximal to splenic flexure; diagnostic, with or without collection of specimen (s) by brushing or washing, with or without colon decompression (separate procedure) G0121 ( colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk.
What are the global periods for colonoscopy?
Typically, procedure codes with 0, 10 or 90-day global periods include pre-work, intraoperative work, and post-operative work in the Relative Value Units (RVUs) assigned . As a result, CMS’ policy does not allow for payment of an Evaluation and Management (E/M) service prior to a screening colonoscopy. In 2005, the Medicare carrier in Rhode Island explained the policy this way:
What word is used for colonoscopy screening?
In this case, since the word SURVEILLANCE colonoscopy is documented, I would recommend coding this as a screening (Z12.11), followed by any findings, as well as the personal history of colonic polyps (Z86.010) – sequenced in that order.
What is the code for colon polyp removal?
Remember that once the polyp is removed the patient follow up visits should not be code with K63.5, polyp of colon. Then, use code Z86.010, personal history of colonic polyps.
Why do you need a screening code?
A screening code may be a first-listed code if the reason for the visit is specifically the screening exam. It may also be used as an additional code if the screening is done during an office visit for other health problems. A screening code is not necessary if the screening is inherent to a routine examination, such as a pap smear done during a routine pelvic examination.
What is a screening mammogram?
A screening mammogram is an example of such a test. If a screening examination identifies pathology, the code for the reason the test (namely, the screening code from categories Z11-Z13) is assigned as the principle diagnosis or first-listed code, followed by a code for the pathology or condition found during the screening exam.”.
What is 21c screening?
I 21 c Screening is the testing for disease or disease precursors in seemingly well individuals so that early detection and treatment can be provided for those who test positive for the disease (e.g., screening mammogram).
What is the purpose of a test to rule out a suspected diagnosis?
In these cases, the sign or symptom is used to explain the reason for the test.
Is colon cancer a screening?
A: Of note, if there is only a diagnosis of FAMILY history of colon cancer and nothing else is documented, these are coded as a screening (even if the physician doesn’t document screening). This is based on a Coding Clinic, 1999, 1st qtr. page 4.
What are the two types of ICD-9 codes?
According to ICD-9-CM Official Guidelines for Coding and Reporting, section 18.d.4:#N#There are two types of history V codes, personal and family . Personal history codes explain a patient’s past medical condition that no longer exists and is not receiving any treatment, but that has the potential for recurrence, and therefore may require continued monitoring. Personal history codes may be used in conjunction with follow-up codes and family history codes may be used in conjunction with screening codes to explain the need for a test or procedure.#N#Common personal history codes used with colonoscopy are V12.72 and V10.0x Personal history of malignant neoplasm of the gastrointestinal tract. The family history codes include V16.0 Family history of malignant neoplasm of the gastrointestinal tract; V18.51 Family history of colonic polyps; and V18.59 Family history of other digestive disorders. Lastly, V76.51 describes screening of the colon.#N#Per the ICD-9-CM official guidelines, you would be able to report V76.51 (screening) primary to V16.0 (family history of colon polyps). In contrast, you would not use V76.51 (screening) with V12.72 (personal history of colon polyps) because family history codes, not personal history codes, should be paired with screening codes. Personal history would be paired with a follow-up code.#N#Just because you get paid doesn’t mean the coding is correct: Most carriers will pay V76.51 with V12.72 because their edits are flawed and allow it. The patient’s claim will process under a patient’s preventative benefits with no out-of-pocket; however, an audit of the record with the carrier guidance will reveal that the claim incorrectly paid under preventative services when, in fact, the procedure should have paid as surveillance. The best strategy is to contact your payer to be sure you are coding correctly based on that payer’s “screening vs. surveillance” guidelines.
How often should a colonoscopy be performed?
Preventive Services Task Force (USPSTF):#N#A screening colonoscopy is performed once every 10 years for asymptomatic patients aged 50-75 with no history of colon cancer, polyps, and/or gastrointestinal disease.#N#A surveillance colonoscopy can be performed at varying ages and intervals based on the patient’s personal history of colon cancer, polyps, and/or gastrointestinal disease. Patients with a history of colon polyp (s) are not recommended for a screening colonoscopy, but for a surveillance colonoscopy. Per the USPSTF, “When the screening test results in the diagnosis of clinically significant colorectal adenomas or cancer, the patient will be followed by a surveillance regimen and recommendations for screening are no longer applicable.”#N#The USPSTF does not recommend a particular surveillance regime for patients who have a personal history of polyps and/or cancer; however, surveillance colonoscopies generally are performed in shortened intervals of two to five years. Medical societies, such as the American Society of Colon and Rectal Surgeons and the American Society of Gastrointestinal Endoscopy, regularly publish recommendations for colonoscopy surveillance.#N#The type of colonoscopy will fall into one of three categories, depending on why the patient is undergoing the procedure.#N#Diagnostic/Therapeutic colonoscopy (CPT® 45378 Colonoscopy, flexible, proximal to splenic flexure; diagnostic, with or without collection of specimen (s) by brushing or washing, with or without colon decompression (separate procedure))#N#Patient has a gastrointestinal sign, symptom (s), and/or diagnosis.#N#Preventive colonoscopy screening (CPT® 45378, G0121 Colorectal cancer screening; colonoscopy on individual not meeting criteria for high risk)#N#Patient is 50 years of age or older#N#Patient does not have any gastrointestinal sign, symptom (s), and/or relevant diagnosis#N#Patient does not have any personal history of colon cancer, polyps, and/or gastrointestinal disease#N#Patient may have a family history of gastrointestinal sign, symptom (s), and/or relevant diagnosis#N#Exception: Medicare patients with a family history (first degree relative with colorectal and/or adenomatous cancer) may qualify as “high risk.” Colonoscopy for these patients would not be a “surveillance,” but a screening, reported with HCPCS Level II code G0105 Colorectal cancer screening; colonoscopy on individual at high risk.#N#Surveillance colonoscopy (CPT® 45378, G0105)#N#Patient does not have any gastrointestinal sign, symptom (s), and/or relevant diagnosis.#N#Patient has a personal history of colon cancer, polyps, and/or gastrointestinal disease.
How to avoid confusion during colonoscopy?
To avoid angry, confused patients, educate them about the types of colonoscopy (preventative, surveillance, or diagnostic) and insurance benefits associated with each procedure . Accomplish this by providing the patient with the correct tools.
Which medical societies publish recommendations for colonoscopy surveillance?
Medical societies, such as the American Society of Colon and Rectal Surgeons and the American Society of Gastrointestinal Endoscopy, regularly publish recommendations for colonoscopy surveillance. The type of colonoscopy will fall into one of three categories, depending on why the patient is undergoing the procedure.
Is there an increase in colonoscopy codes?
Practices performing colonoscopies for colon and rectal cancer screenings have seen a corresponding rise in requests for “screening” colonoscopy. As a result, there is an increase in incorrectly coded colonoscopies. Practices may not understand that a majority of patients are actually not screening colonoscopies, ...
Is colonoscopy a screening?
Colonoscopy for these patients would not be a “ surveillance,” but a screening, reported with HCPCS Level II code G0105 Colorectal cancer screening; colonoscopy on individual at high risk. Patient does not have any gastrointestinal sign, symptom (s), and/or relevant diagnosis.
Does the ACA cover colonoscopy?
Under the ACA, payers must offer first-dollar coverage for screening colonoscopy but are not obliged to do so for a surveillance or diagnostic colonoscopy. The patient’s history and findings determine the reason for and type of colonoscopy, driving the benefit determination.
What is the HCPCS code for colonoscopy?
For Medicare beneficiaries, screening colonoscopy is reported using the following HCPCS codes: - G0105 (Colorectal cancer screening; colonoscopy on individual at high risk), for a Medicare beneficiary at high risk for colorectal cancer, and the appropriate diagnosis code that necessitates the more frequent screening.
What is the ICD-10 code for colonoscopy without biopsy?
Point to note: Code 45378 is the base code for a colonoscopy without biopsy or other interventions. It includes brushings or washings if performed. Report 45378 with ICD-10 code Z86.010 on the first line of the CMS 1500 form.
How often does Medicare require colonoscopy?
Medicare beneficiaries without high-risk factors are eligible for a screening colonoscopy every ten years. Beneficiaries at higher risk for developing colorectal cancer are eligible for screening once every 24 months. Medicare considers an individual who is at high risk of developing colorectal cancer as one who has one or more of the following:
How effective is colonoscopy?
According to a study by the American Cancer Society, 90% colorectal cancer (CRC) cases are detected in individuals with over 50 years in the U.S and colonoscopy is the most effective and the most commonly adopted procedure for the diagnosis and screening of CRC in older adults.
Why do you need a colonoscopy?
A Screening colonoscopy is performed on person without symptoms in order to test for the presence of colorectal cancer or colorectal polyps. Even if a polyp or cancer is found during a screening exam, it does not change the screening intent.
What is colonoscopy examination?
CPT defines a colonoscopy examination as "the examination of the entire colon, from the rectum to the cecum or colon-small intestine anastomosis, and may include an examination of the terminal ileum or small intestine proximal to an anastomosis" as well.
When should modifier 33 be appended?
33 - Modifier 33 modifier should be appended for preventive services when the primary purpose of the service is the delivery of an evidence-based service.
What is a bill and coding article?
Billing and Coding articles provide guidance for the related Local Coverage Determination (LCD) and assist providers in submitting correct claims for payment. Billing and Coding articles typically include CPT/HCPCS procedure codes, ICD-10-CM diagnosis codes, as well as Bill Type, Revenue, and CPT/HCPCS Modifier codes. The code lists in the article help explain which services (procedures) the related LCD applies to, the diagnosis codes for which the service is covered, or for which the service is not considered reasonable and necessary and therefore not covered.
Is Z80.0 a covered ICD-10 code?
Note: Z80.0 does not appear as a covered ICD-10 code in the Billing and Coding: Colonoscopy/Sigmoidoscopy/Proctosigmoidoscopy A56632 article because the Colonoscopy/Sigmoidoscopy/Proctosigmoidoscopy L34454 LCD addresses ONLY procedures performed for diagnostic and/or therapeutic purposes. LCD L34454 and Article A56632 do not address criteria for the performance of or coding for screening procedures or screening procedures that are converted to diagnostic/therapeutic procedures based upon unanticipated pathology encountered during the visualization of the colon.
Is CPT a year 2000?
CPT is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to, the implied warranties of merchantability and fitness for a particular purpose. AMA warrants that due to the nature of CPT, it does not manipulate or process dates, therefore there is no Year 2000 issue with CPT. AMA disclaims responsibility for any errors in CPT that may arise as a result of CPT being used in conjunction with any software and/or hardware system that is not Year 2000 compliant. No fee schedules, basic unit, relative values or related listings are included in CPT. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this file/product is with CMS and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this file/product. This Agreement will terminate upon no upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
Can you use CPT in Medicare?
You, your employees and agents are authorized to use CPT only as contained in the following authorized materials of CMS internally within your organization within the United States for the sole use by yourself, employees and agents. Use is limited to use in Medicare, Medicaid or other programs administered by the Centers for Medicare and Medicaid Services (CMS). You agree to take all necessary steps to insure that your employees and agents abide by the terms of this agreement.
Is CPT copyrighted?
CPT codes, descriptions and other data only are copyright 2020 American Medical Association. American Medical Association. All Rights Reserved (or such other date of publication of CPT). CPT is a trademark of the American Medical Association (AMA).
Does CMS have a CDT license?
Organizations who contract with CMS acknowledge that they may have a commercial CDT license with the ADA, and that use of CDT codes as permitted herein for the administration of CMS programs does not extend to any other programs or services the organization may administer and royalties dues for the use of the CDT codes are governed by their commercial license.
When will the ICD-10 Z12.11 be released?
The 2022 edition of ICD-10-CM Z12.11 became effective on October 1, 2021.
What is screening for asymptomatic disease?
Screening is the testing for disease or disease precursors in asymptomatic individuals so that early detection and treatment can be provided for those who test positive for the disease. Type 1 Excludes. encounter for diagnostic examination-code to sign or symptom. Use Additional.
Popular Posts:
- 1. icd-9 code for intermittent chest pain
- 2. icd-10-cm code for pneumonia due to food aspiration
- 3. in the icd-10-cm manual the code range t80-t88 is used for:
- 4. icd 9 code for impending respiratory failure
- 5. icd-10 code for malnutrition
- 6. icd 10 code for hardware removal left tibia
- 7. what's the icd 10 code for old sacroiliac joint lesion
- 8. icd 10 cm code for cervical lymph node enlarged and tender bilaterally
- 9. what is the icd 19 code for nasal verruca vulgaris
- 10. icd 10 code for facial contusion initial encounter