86.11
What is the diagnosis code for skin biopsy?
2012 ICD-9-CM Procedure Code 86.1 Diagnostic Procedures On Skin And Subcutaneous Tissue A child code below 86.1 with greater detail should be used. 2012 ICD-9-CM Procedure Code 86.11 Closed Biopsy Of Skin And Subcutaneous Tissue 86.11 is a specific code and is valid to identify a procedure. 2012 ICD-9-CM Procedure Code 86.19
What is the diagnosis code for suspicious skin lesion?
7 rows · · Code: Description: 11102. Tangential biopsy of skin (e.g., shave, scoop, saucerize, curette) ...
What is the ICD - 10 PCs code for biopsy?
· 11104 – Punch biopsy of skin (including simple closure, when performed) single lesion. +11105 – Each separate/additional lesion (List separately in addition to code for primary procedure. 11106 – Incisional biopsy of skin (including …
What is the code for biopsy of mole on skin?
· What diagnosis code should you use when sending a skin biopsy to pathology? a) D48.5 Neoplasm of uncertain behavior of skin, or b) D49.2 Neoplasm of unspecified behavior of bone, soft tissue, and skin Answer: The answer is b! Use an unspecified code when a specific diagnosis code is not known at the time of encounter.
What is the ICD-10 code for skin biopsy?
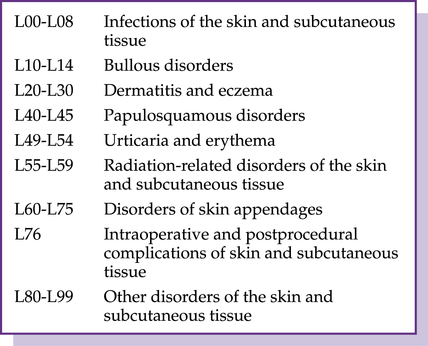
ICD-10-CM Code(s): L98. 8 Other specified disorders of the skin and subcutaneous tissue.
What is the CPT code for punch biopsy of skin lesion?
11104NEW BIOPSY CODESCPT codeDescriptionGlobal days11104Punch biopsy of skin (including simple closure, when performed), single lesion0+11105Each additional lesionN/A11106Incisional biopsy of skin (e.g., wedge; including simple closure, when performed), single lesion0+11107Each additional lesionN/A2 more rows
How do you code punch biopsy?
Punch biopsies (codes 11104-11105) use a punch tool to remove a full thickness cylindrical sample of the skin. Incisional biopsies (codes 1106-11107) use sharp blade to remove a full thickness sample of tissue via a vertical incision or wedge, penetrating deep to the dermis and into the subcutaneous space.
What is the ICD-10 code for skin lesion?
ICD-10-CM Code for Disorder of the skin and subcutaneous tissue, unspecified L98. 9.
How do you code a biopsy?
Prior to the new CPT codes for 2019, biopsies were reported with CPT code 11100 for the first lesion and 11101 for each additional lesion biopsied regardless of method of removal. The new biopsy codes are reported based on method of removal including: Tangential biopsy (11102 and 11103) Punch biopsy (11104 and 11105)
How do you code a 3 punch biopsy?
The coder should report CPT code 11106 for the primary procedure, as this describes an incisional biopsy, and add-on codes 11105 and 11103 for the punch and tangential biopsies, respectively.
What is CPT code for skin biopsy?
CPT deleted skin biopsy code 11100 and add-on code 11101 this year and introduced three base codes and three add-on codes that are defined by the method of biopsy — tangential, punch, or incisional — rather than size or anatomic location.
What is the CPT code for biopsy of soft tissue?
1110011100: Biopsy of skin, subcutaneous tissue and/or mucous membrane (including simple closure), unless otherwise listed; single lesion.
How do you code an excisional biopsy?
Answer: No, CPT does not have a code for excisional biopsy. It is either a biopsy (11100 or 11101) or a benign or malignant excision code. (114xx, 116xx).
What is skin and subcutaneous tissue disorders?
Panniculitis. Panniculitis is a group of conditions that causes inflammation of your subcutaneous fat. Panniculitis causes painful bumps of varying sizes under your skin. There are numerous potential causes including infections, inflammatory diseases, and some types of connective tissue disorders like lupus.
What is the ICD-10 code for disorder of the skin and subcutaneous tissue unspecified?
ICD-10 code: L98. 9 Disorder of skin and subcutaneous tissue, unspecified.
What is the ICD-10 code for skin nodule?
R222022 ICD-10-CM Diagnosis Code R22: Localized swelling, mass and lump of skin and subcutaneous tissue.
When to use unspecified code?
The answer is b! Use an unspecified code when a specific diagnosis code is not known at the time of encounter.
When is it appropriate to report codes for sign and symptom?
The general guidelines say, “If a definitive diagnosis has not been established by the end of the encounter, it is appropriate to report codes for sign (s) and/or symptom (s) in lieu of a definitive diagnosis.”. This is exactly the situation when a biopsy is taken and sent for pathology. This is confirmed in the general guidelines related ...
What does D48 mean?
D48. These classify the neoplasm by site and should be used when “i.e., histologic confirmation whether the neoplasm is malignant or benign cannot be made.”. Unspecified, on the other hand, means that a definitive diagnosis cannot be made at the time of the encounter. The general guidelines say,
What is an uncertain neoplasm?
An uncertain neoplasm is reported after the pathologist’s report, not when sending the specimen for biopsy. According to ICD-10, there are specific categories of codes that are used for neoplasms of uncertain behavior. They are:
Is a benign neoplasm in the body system?
Certain benign neoplasms, such as prostatic ade nomas, may be found in the specific body system chapters. To properly code a neoplasm it is necessary to determine from the record if the neoplasm is benign, in-situ, malignant, or of uncertain histologic behavior.”. The word uncertain is related to a histologic determination.
What is the procedure code for biopsy?
According to the AMA, "The use of a biopsy procedure code (e.g., 11102, 11103) indicates that the procedure to obtain tissue for pathologic examination was performed independently, or was unrelated or distinct from other procedures/services provided at that time."
What is the biopsy code for a lesion?
If only a portion of a lesion is removed to determine its pathology, you should use a biopsy code 11102 - 11103. If the entire lesion is removed, you also have the option of reporting the shave removal codes 11300 - 11313 and excision codes for lesions 11400 - 11646, even if the lesion was sent to pathology.
How many codes should be reported for a large lesion?
If a large lesion is sampled at several separate locations or sites using a single biopsy code, then only one code should be reported.
What is tangential biopsy?
Tangential Biopsy 11102, 11103#N#Performed with a sharp blade (e.g., shave, scoop, saucerize, curette) like a flexible biopsy blade, obliquely oriented scalpel, or a curette to remove a sample of epidermal tissue, this can be with or without portions of the underlying dermis. Removal of skin tags uses a different set of codes ( 11200, 11201 ), not to be confused with lesions. Therapeutic removal using a shave technique can also be done as a tangential biopsy using CPT codes 11300 - 11313; these are reported for reasons such as a symptomatic lesion that rubs on a waistband or bra. The provider must indicate the purpose of the procedure.
Can biopsies be reported?
Any combination of biopsies can be reported if applicable, as in this example:
What is skin lesion?
A skin lesion is a general term used to describe any change in the skin surface, and it can occur on any area of the body, according to Aetna. A skin lesion may present with various characteristics including raised, flat, large, small, fluid-filled, or with color.
What are the different types of skin cancer?
According to the American Cancer Society, the three main types of malignant skin lesions, or skin cancer, are basal cell carcinoma, squamous cell carcinoma, and melanoma.
What are the common benign skin tumors?
Common benign skin tumors include moles (nevi), seborrheic keratoses, skin tags (acrochordon), sebaceous cysts, corns, warts (verruca vulgaris), and callouses . Premalignant (Precancerous) Lesions or Neoplasms. A premalignant lesion is a lesion that may become malignant in time or may be in the early stages of skin cancer.
What are the different types of lesions?
The different types of lesions are benign, premalignant, and malignant.
What is the code for excisional biopsy?
Be sure to document the location and size of each lesion. Excisional biopsies include two sets of codes, for excision of benign lesions (codes 11400–11471) or malignant lesions (codes 11600–11646).
What is the code for a shave biopsy?
Here are some reminders for those codes. Shave biopsies (codes 11300–11313) use a sharp instrument to remove epidermal or dermal lesions without a full-thickness excision. They are used for therapeutic removal when the lesion is symptomatic, such as rubbing on a waist band or bra line.
How many lesions can you treat with 17110?
For the destruction of benign lesions (seborrheic keratoses and warts), bill a single unit of code 17110 to treat up to 14 lesions and a single unit of code 17111 for 15 or more.
What is the add on code for multiple biopsies?
If multiple biopsies are performed using different techniques, report the primary code with the highest RVUs, then use the add-on code that is specific to the other biopsies performed. When billing for these services, record the method and the number of units in your documentation.
When did the CPT change the codes for tangential biopsy?
CPT created new codes in 2019 for tangential, punch, and incisional biopsies and deleted two old biopsy codes. Codes for shave and excisional biopsies, as well as destruction of benign, premalignant, and malignant lesions and skin tags, have not changed. When performing multiple skin procedures for the same patient on the same day, ...
Can you code multiple skin procedures?
Correct coding for skin procedures is not impossible. This article will detail how to code for two types of common skin procedures — biopsies and destruction of lesions — as well as how to code when multiple skin procedures are performed on the same day. The “ Skin care encounter form ” features codes for the skin procedures most commonly performed by family physicians.
Is it easier for a family physician to perform skin procedures than it is to correctly code for them?
Enlarge. It is often easier for family physicians to perform skin procedures than it is to correctly code for them. The codes are complicated, and many electronic health record systems and even the CPT manual use different terms than physicians use to describe these services.
What is the diagnosis code for neoplasm of uncertain behavior of skin?
My research suggests that most dermatologists tend to use the diagnosis code for neoplasm of uncertain behavior of skin (238.2) when biopsying or shaving a lesion of uncertain etiology because of concern about malignancy and billing before the histopathology is known.
What is the BCC code for dermatosis?
If you biopsy three different lesions, or three different areas of a dermatosis, then the code is 11100 for the first biopsy and +11101 for each additional biopsy. However, if you do shaves and curettage with curative intent, wait for the pathology to return to verify BCC.
Does Medicare cover removal of lesions?
When a patient asks for removal of a lesion for cosmetic reasons, Medicare, Medicaid, and most other insurance plans do not cover the service. Billing insurance for cosmetic removal of lesions could be deemed fraudulent. Tell the patient before the procedure that it may result in an out-of-pocket expense.
Can you excise seborrheic keratoses?
It is almost always inappropriate to excise seborrheic keratoses when you are certain of the diagnosis. It is often appropriate to remove them because of symptoms, but only via the shave technique. Note that for smaller lesions, biopsy codes may provide greater reimbursement than shave codes. Lines can be blurred.
Can you upcode destruction of benign lesions?
4. Don't upcode destruction of benign lesions or undercode destruction of malignancies
What is the code for skin biopsies?
For many years we have used two codes to report skin biopsies. CPT® 11100 for the first lesion and 11101 for each additional lesion biopsied after the first lesion on the same date of service.
What is partial thickness biopsies?
The CPT Guidelines state: “Partial-thickness biopsies are those that sample a portion of the thickness of skin or mucous membrane and do not penetrate below the dermis or lamina propria, full-thickness biopsies penetrate tissue deep to the dermis or lamina propria, into the subcutaneous or submucosal space.
What is a punch biopsy?
Punch Biopsy. A punch biopsy required a punch tool to remove a full thickness cylindrical sample of the skin. The intent of the biopsy is to remove a sample of a cutaneous lesion for a diagnostic pathologic examination. Simple closure is include and cannot be billed separately.
Is a skin lesion considered a biopsy?
When a skin lesion is entirely removed, either by excision or shave removal and sent to pathology for examination, it is not considered a biopsy for coding purposes but an excision and should be reported with the excision codes not biopsy CPT codes.
Is simple closure included in a biopsy?
Simple closure is include and cannot be billed separately. Incisional Biopsy. An incisional biopsy requires the use of a sharp blade (not a punch tool) to remove a full-thickness sample of tissue via a vertical incision or wedge, penetrating deep to the dermis, into the subcutaneous space.
Popular Posts:
- 1. icd 9 code for soft tissue injury
- 2. icd 10 code for foul smelling urine
- 3. icd 10 code for gun shot
- 4. icd 10 code for calcification density abdomen
- 5. icd 10 code for right sided hemiparesis
- 6. icd 10 cm code for viral
- 7. icd 10 code for torn lateral meniscus right knee
- 8. icd 10 code for lower extremity feet neuropathy
- 9. 2019 icd 10 code for new leukopenia
- 10. icd 9 code for enlarged lymph nodes