ICD-10 | Neoplasm related pain (acute) (chronic) (G89. 3)
What is the diagnosis code for pain?
ICD-9 DIAGNOSIS ICD-10 DIAGNOSIS 724.1 Pain in thoracic spine M54.6 Pain in thoracic spine 724.2 Lumbago M54.5 Low back pain 725.4 Backache, unspecified M54.89 Other dorsalgia ...
What is the ICD - 9 code for pain?
Pain in joint, ankle and foot Short description: Joint pain-ankle. ICD-9-CM 719.47 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, 719.47 should only be used for claims with a date of service on or before September 30, 2015.
What is the CPT code for pain?
We have a pain clinic physician who is wanting to report the new CPT 64486 TAPS by single injection for chronic pain management of the transverse abdominus. Since 64486 seems to be indicated for post op pain management I believe that CPT 64450 injection other peripheral nerve would be a better choice.
Where can one find ICD 9 diagnosis codes?
ICD-9 Codes . While phased out in 2015, you will still see ICD-9 codes on older documents. Most ICD-9 codes are three digits to the left of a decimal point and one or two digits to the right of one. For example:
What is the ICD-10 designation for pain?
ICD-10 code R52 for Pain, unspecified is a medical classification as listed by WHO under the range - Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
How do you code neoplasm pain?
Neoplasm-Related Pain Code 338.3 is used to classify pain related to, associated with, or due to a tumor or cancer whether primary or secondary. This code is used as the principal code when the admission or encounter is for pain control or pain management.
What is neoplasm pain?
Neoplasm related pain (acute) (chronic): ICD-9-CM Code 338.3. Definition: Pain in body part/region as a direct result of a neoplasm which is a recognized allowed condition in the claim. Pain must significantly impacts activity and requires ongoing medical treatment directed toward relief of pain.
What is the ICD-10-CM code for chronic pain?
NOTE: To utilize these chronic pain diagnosis codes, the exact nature of pain should be specifically documented in the patient medical records; such as “chronic” to utilize ICD-10 code G. 89.29 or the diagnosis term “chronic pain syndrome” to utilize ICD-10 code G89. 4.
How do you code chronic pain?
You should code this condition only when the physician specifically documents it. Chronic pain syndrome is reported with code G89. 4 (Chronic pain syndrome). ICD-10 implementation is now less than two years away.
Can chronic pain be a primary diagnosis?
Only report pain diagnosis codes from the G89 category as the primary diagnosis when: The acute or chronic pain and neoplasm pain provide more detail when used with codes from other categories; or. The reason for the service is for pain control or pain management.
What are the different types of pain?
The five most common types of pain are:Acute pain.Chronic pain.Neuropathic pain.Nociceptive pain.Radicular pain.
What is the definition of neuropathic pain?
Neuropathic pain is now defined by the International Association for the Study of Pain (IASP) as 'pain caused by a lesion or disease of the somatosensory nervous system'.
What is Neuroplastic pain?
Neuroplasticity and chronic pain This is a phenomenon associated with changes at the nervous tissue which amplifies pain signal transmission to the brain.
What does diagnosis code M54 9 mean?
9: Dorsalgia, unspecified.
What is the ICD-10 code for M54 50?
M54. 50, Low back pain, unspecified.
Coding Notes for G89.3 Info for medical coders on how to properly use this ICD-10 code
Inclusion Terms are a list of concepts for which a specific code is used. The list of Inclusion Terms is useful for determining the correct code in some cases, but the list is not necessarily exhaustive.
ICD-10-CM Alphabetical Index References for 'G89.3 - Neoplasm related pain (acute) (chronic)'
The ICD-10-CM Alphabetical Index links the below-listed medical terms to the ICD code G89.3. Click on any term below to browse the alphabetical index.
Equivalent ICD-9 Code GENERAL EQUIVALENCE MAPPINGS (GEM)
This is the official exact match mapping between ICD9 and ICD10, as provided by the General Equivalency mapping crosswalk. This means that in all cases where the ICD9 code 338.3 was previously used, G89.3 is the appropriate modern ICD10 code.
What is the code for flank pain?
You must code flank pain as unspecified abdominal pain (R10.9) unless the physician provides additional information about the location of the pain, such as whether it is in the upper or lower portion of the abdomen. Pelvic pain is classified to code R10.2 (Pelvic and perineal pain).
What is the code for abdominal pain?
In addition to the codes for pain in the various parts of the abdomen, there are codes for: Acute abdomen (R10.0): This is sudden, severe abdominal pain, often accompanied by rigidity of the abdomen.
What is the ICd 10 code for post thoracotomy pain?
Category G89 contains four codes for acute and chronic post-thoracotomy pain (G89.12, G89.22) and other postprocedural pain (G89.18, G89.28). The ICD-10-CM guidelines state that you should not code “routine or expected postoperative pain immediately after surgery.” Additionally, in order to assign these codes, the physician must document that the patient’s pain is a complication of the surgery.
What is the G89 code?
For example, you can assign a G89 code to indicate that the pain is acute or chronic. You should assign the site-specific pain code first unless the purpose of the encounter is pain management, in which case the G89 code is first. For example, a patient is referred for ankle x-rays for chronic right ankle pain.
What is R07.81 pain?
Pleurodynia (R07.81): Spasms of pain in the intercostal muscles, which can be a sign of pleurisy (inflammationof the pleural membranes). Intercostal pain (R07.82): This is pain originating in the intercostal nerves, which run between pairs of adjacent ribs.
What is a pain that does not point to a specific body system?
Pain that does not point to a specific body system is classified in the Symptoms and Signs chapter. For example, abdominal pain is classified to category R10. Certain specific types of pain are classified to category G89 (Pain, not elsewhere classified) in the Nervous System chapter.
What is Category G89?
Category G89 contains codes for acute (G89.11) and chronic (G89.21) pain due to trauma. You should not assign these codes if a cause for the pain (i.e., a specific injury) has been identified, except in the unlikely event that the purpose of the encounter is pain management.
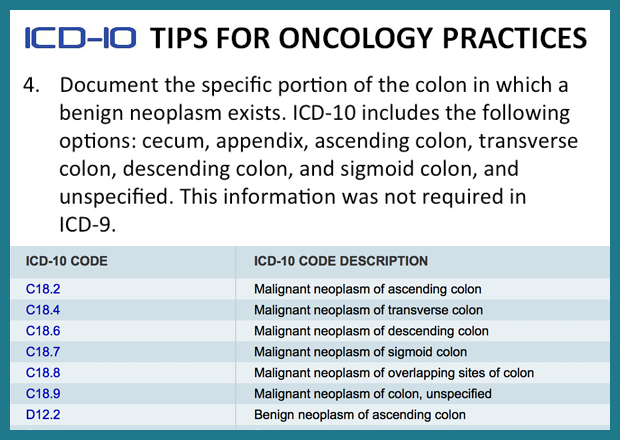
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion '), unless the combination is specifically indexed elsewhere. For multiple neoplasms of the same site that are not contiguous such as tumors in different quadrants of the same breast, codes for each site should be assigned.
What is the Z85 code for a primary malignancy?
When a primary malignancy has been previously excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy at that site, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy. Any mention of extension, invasion, or metastasis to another site is coded as a secondary malignant neoplasm to that site. The secondary site may be the principal or first-listed with the Z85 code used as a secondary code.
What is Chapter 2 of the ICD-10-CM?
Chapter 2 of the ICD-10-CM contains the codes for most benign and all malignant neoplasms. Certain benign neoplasms , such as prostatic adenomas, may be found in the specific body system chapters. To properly code a neoplasm, it is necessary to determine from the record if the neoplasm is benign, in-situ, malignant, or of uncertain histologic behavior. If malignant, any secondary ( metastatic) sites should also be determined.
What is C80.0 code?
Code C80.0, Disseminated malignant neoplasm, unspecified, is for use only in those cases where the patient has advanced metastatic disease and no known primary or secondary sites are specified. It should not be used in place of assigning codes for the primary site and all known secondary sites.
When a pregnant woman has a malignant neoplasm, should a code from subcatego
When a pregnant woman has a malignant neoplasm, a code from subcategory O9A.1 -, malignant neoplasm complicating pregnancy, childbirth, and the puerperium, should be sequenced first, followed by the appropriate code from Chapter 2 to indicate the type of neoplasm. Encounter for complication associated with a neoplasm.
What is the code for leukemia?
There are also codes Z85.6, Personal history of leukemia, and Z85.79, Personal history of other malignant neoplasms of lymphoid, hematopoietic and related tissues. If the documentation is unclear as to whether the leukemia has achieved remission, the provider should be queried.
What is C80.1?
Code C80.1, Malignant ( primary) neoplasm, unspecified, equates to Cancer, unspecified. This code should only be used when no determination can be made as to the primary site of a malignancy. This code should rarely be used in the inpatient setting.
What is the ICD 11 for pain?
An inside look at the ICD-11's integration of chronic pain, including expanded criteria for neuropathic pain. The World Health Organization (WHO) released a preliminary version of the 11th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-11) in June 2018.
What is the ICd 11 for neuropathic pain?
14,15 The current release of ICD-11 is limited to brief summary descriptions of central and peripheral neuropathic pain. 1 Figure 2 shows the complete list of entities that will ultimately be incorporated under these headings. Each entry will contain information on the underlying etiology, the clinical phenotype of pain, and suitable additional investigations to support the diagnosis of neuropathic pain. The entries will specify distinct criteria for possible, probable, or definite neuropathic pain following the recommendations of NeuPSIG. 14,15
What is the difference between fibromyalgia and irritable bowel syndrome?
Fibromyalgia is one of the entities characterized by chronic widespread pain while irritable bowel syndrome is an example of chronic primary visceral pain. The chronic primary headaches listed in ICD-11 comprise migraine, tension-type headache, and trigeminal autonomic cephalalgias, matching those included in the third edition ...
When will the ICD-11 be adopted?
The World Health Assembly is expected to vote on the adoption of the final version of ICD-11 in May 2019 ( Editor's note: The WHA officially adopted the ICD-11 on May 25, 2019; to take effect in January 2022.) It is expected that its ultimate implementation by member states of the WHO will take time.
Is chronic pain a symptom?
Although chronic pain is a symptom, it requires diagnostic evaluation and management efforts on a scale that calls for the inclusion of a systematic classification of disorders associated with persistent or recurrent pain in the I CD.
What is cancer related pain?
Chronic cancer-related pain is chronic pain caused by theprimary cancer itself or metastases (chronic cancer pain) or itstreatment (chronic postcancer treatment pain). It is distinct frompain caused by comorbid disease. Pain in cancer survivors mustbe monitored carefully because a change in pain quality orintensity can indicate recurrence of the initial malignancy. Carefulassessment is required to distinguish pain caused by cancer frompain caused by cancer treatment or comorbid conditions. It iscommon for these pains to be concurrent, eg, thoracic surgery fora lung cancer might cause postsurgical pain, which can be
What is the pain of a neuropathic cancer?
Chronic neuropathic cancer pain is chronic pain caused by a primarytumour or metastases damaging or injuring the peripheral or centralnervous system.42 Examples of chronic peripheral neuropathiccancer pain include thoracic tumour or metastases damaging thebrachial plexus or abdominal or pelvic cancers damaging thelumbosacral plexus. Spinal cord compression (from collapsedvertebral boney metastases) can result in chronic central neuro-pathic cancer pain. Chronic neuropathic cancer pain may beassociated with distinct symptom descriptors,34and the pain istypically perceived in the distribution of affected nerves. Neuropathicmechanisms are associated with poorer outcomes in cancer pain.39It is important to identify correctly the neuropathic mechanisms toguide the use of additional analgesic treatment.35
What is the first line of treatment for cancer?
first line treatment for many cancers is surgery to remove thecancer or the metastases. Because surgery-related chronic painwill be the same regardless whether the surgery is related to canceror to some other condition, chronic postcancer surgery pain will becoded alongside other chronic postsurgical pain according to thetype of surgery in the section on postsurgical pain. This will alsoinclude chronic pain after biopsy or from a chest or abdominal draininsertion for pleural effusion or peritoneal ascites.43Chronic postcancer surgery pain is particularly commonafter treatment for breast (postmastectomy pain) or lungcancer (post-thoracotomy pain) but can follow any cancersurgery or surgical procedure (eg, a tissue biopsy or insertionof a thoracic drain). At 9 months after mastectomy, 63% ofwomen reported persistent pain that was moderate to severein 25% of the whole sample.8 After thoracotomy for lungcancer, 33% reported pain at 3 years after surgery, which wasmoderate to severe in 11% to 18% of the whole sample.51Thepredominant mechanism of postsurgical pain is likely to beneuropathic but not exclusively so.50
What is the pain caused by radiation?
It is probably caused by nerve compression asa consequence of radiation-induced fibrosis, but direct injury tonerves and blood vessels is also likely after microvascularischaemia.12,13It usually occurs several years after radiother-apy and is often progressive and irreversible. The most frequentand best-known form of radiation-induced neuropathy isbrachial plexopathy,18which may follow irradiation for breastcancer or apical lung cancer. However, painful lumbosacralplexopathy after pelvic radiotherapy and axial neuropathy of thespinal cord after cervical radiotherapy have also been de-scribed.14 Chronic painful polyneuropathy is a secondarydiagnosis.42parent for this
What is post radiation pain?
Chronic postradiotherapy pain is chronic pain caused by delayedlocal damage to the nervous system, bones, or other soft tissuesin the field of radiotherapy given to treat the primary tumour ormetastases. Chronic postradiotherapy pain is rare, but itsoccurrence is better recognized with improved long-term cancersurvival.12,25Onset can be within a few months of the end ofradiotherapy or up to several years later. Risk factors include largeoverall treatment dose, large dose per radiotherapy treatment,and combined treatment with surgery or chemotherapy.Although overall the incidence is falling, nevertheless, about 2%of breast cancer survivors and up to 15% of head and neckcancer survivors can experience this type of pain.12Pain fromcancer recurrence should be excluded before making thisdiagnosis. The most recognized form of postradiotherapy painis chronic radiation-induced neuropathy, which is described in
What is bone cancer pain?
Chronic bone cancer pain is chronic pain caused by the primarytumour or metastases damaging or injuring boney skeleton, and itis the most common type of chronic cancer pain.33Metasta sesfrom other cancer sites are the most common form of chronicbone cancer pain as primary bone tumours are rare. Examplesinclude an isolated metastasis to femoral shaft from colon cancer,or multiple metastases from breast or prostate cancer, or multiplemyeloma. The most common sites of metastases are vertebrae,pelvis, long bones, and ribs.28A bone metastasis can weakenbone sufficiently such that an innocuous movement, bump, or fallmay result in a pathological fracture.
What is chronic pain?
Chronic cancer pain is defined as chronic pain caused by theprimary cancer or metastases. Chronic cancer pain consists ofinflammatory and neuropathic mechanisms as a direct effect oftissue response to the primary tumour or metastases. These arecaused by tumour expansion, which induces tissue damage andrelease of various inflammatory mediators. In addition, the cancercan also compress and destroy a sensory nerve, whichdenervates the target tissue resulting in neuropathic changes.Cancer pain can be considered a type of mixed nociceptive andneuropathic pain, but increasing amounts of evidence suggestadditional unique features indicating that it should be regarded asa separate pain state.16The temporal characteristics of cancer pain will be describedas continuous (background pain) or intermittent (episodic pain).Intermittent pains can be predictable (incident pain), eg, anexacerbation of pain caused by weight bearing or activity(including swallowing, defaecation, coughing, or repeateddressing changes), or unpredictable (spontaneous pain) un-related to movement or activity, eg, colic, stabbing painassociated with nerve injury. Intermittent pains such as thoserelated to single clinical procedures (injections or biopsies) areregarded as acute pains and not included within the chronic painclassification. Chronic cancer pain is subdivided into 4 catego-ries: 3 with distinct aetiologies: visceral, bone and neuro-pathic,11,22,45and the final category as “other.”
Popular Posts:
- 1. icd 10 code for right parietal lobe
- 2. icd 10 code for foreign body granuloma of soft tissue foot injury
- 3. icd 10 code for nerve pain jaw
- 4. icd code for nail removal with matrix
- 5. icd 10 code for long term use of lisinopril
- 6. icd 10 code for unrepaired vsd
- 7. icd 10 pcs code for open surgical resection of brain tumor with insertion of catheter
- 8. icd 10 code for body mass index 33.58
- 9. icd 10 cm code for exacerbation of chest and epigastric pain
- 10. icd 10 code for contact with fireworks