CPT® code 99203: New patient office visit, 30-44 minutes | American Medical Association.
What is the procedure code for office visit?
Oct 01, 2021 · Z01.89 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z01.89 became effective on October 1, 2021. This is the American ICD-10-CM version of Z01.89 - other international versions of ICD-10 Z01.89 may differ.
What is the CPT code for new patient office visit?
Oct 01, 2021 · Z00.00 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. Short description: Encntr for general adult medical exam w/o abnormal findings. The 2022 edition of ICD-10-CM Z00.00 became effective on …
What are office visit CPT codes?
The office and other outpatient visit codes for new patients (99201- 99205) are still recognized for reimbursement by CMS and may be used to report any new patient being seen in your practice. As a result of these changes, there is no distinction between a patient who is referred by a physician or one who is self referred; for Medicare they are both considered a new patient.
What is new patient vs established patient?
CPT® code 99204: New patient office or other outpatient visit, 45-59 minutes. As the authority on the CPT® code set, the AMA is providing the top-searched codes to help remove obstacles and burdens that interfere with patient care.
What is the ICD 10 code for a new patient visit?
Code the initial visit as a new visit, and subsequent treatment visits as established with the E/M code 99211.
What is the difference between 99213 and 99203?
99203 combines the presenting problem (and decision making) of 99213 with the history and physical of 99214. All require four HPI elements except 99213.
What is the ICD code for office visit?
Encounter for administrative examinations, unspecified
Z02. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z02. 9 became effective on October 1, 2021.
Z02. 9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z02. 9 became effective on October 1, 2021.
What is the CPT code for a new patient seen in the office for 35 minutes?
New Patient Office Visit (CPT Codes 99201-99205): Coverage and Documentation Requirements.Feb 7, 2018
How long is a 99203 visit?
Typical times for new patient office visits
| CPT code | Typical time |
|---|---|
| 99202 | 20 minutes |
| 99203 | 30 minutes |
| 99204 | 45 minutes |
| 99205 | 60 minutes |
•
Feb 9, 2018
Is 99203 covered by Medicare?
Medicare and other Insurance are pleased to pay the lesser money to providers if they (the doctors) are willing to under use the CPT code 99214.
...
CPT CODE 2016 Fee 2017 FEE.
...
CPT CODE 2016 Fee 2017 FEE.
| 99201 | $35.96 $43.6 |
|---|---|
| 99203 | $89.52 $108.3 |
| 99204 | $135.38 $165.7 |
| 99205 | $169.54 $208.2 |
| 99211 | $20.07 $19.63 |
What constitutes a new patient visit?
New Patient - A new patient is defined as one who has not received any professional services from a physician or physician group practice (same physician specialty) within the previous 3 years, e.g., evaluation and managment (E/M) services, surgical procedures or other face-to-face services.
What is the difference between ICD-10-CM and ICD-10-PCS?
The main differences between ICD-10 PCS and ICD-10-CM include the following: ICD-10-PCS is used only for inpatient, hospital settings in the U.S., while ICD-10-CM is used in clinical and outpatient settings in the U.S. ICD-10-PCS has about 87,000 available codes while ICD-10-CM has about 68,000.
What is a 99213 office visit?
Office or other outpatient visit for the evaluation and management of an established patient, which requires a medically appropriate history and/or examination and low level of medical decision making.
Which CPT codes listed on the encounter form are reported for new patient office visits?
Codes 99201-99205 apply to new patient visits. The descriptors for all 5 of the codes (99201, 99202, 99203, 99204, and 99205) begin with the same language, including a reference to a new patient: Office or other outpatient visit for the evaluation and management of a new patient ….
When the phone is Sudications 4444 444444444444444444444444444444?
When the sole purpose of the telephone/Internet communication is to arrange a transfer of care or other face-to-face services, the code range 99444-99449 for interprofessional telephone/Internet consultations are not reported.
What is modifier 25 in CPT coding?
Evaluation and Management
The Current Procedural Terminology (CPT) definition of Modifier 25 is as follows: Modifier 25 – this Modifier is used to report an Evaluation and Management (E/M) service on a day when another service was provided to the patient by the same physician or other qualified health care professional.
What is an outpatient visit?
Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician or other qualified health care professional. Usually, the presenting problem (s) are minimal.
What is 99211 in medical terms?
99211. Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician or other qualified health care professional. Usually, the presenting problem (s) are minimal. Typically, 5 minutes are spent performing or supervising these services.
How long is a face to face visit?
Typically, 40 minutes are spent face-to-face with the patient and/or family. Office or other outpatient visit for the evaluation and management of an established patient, which requires a medically appropriate history and/or examination and high level of medical decision making.
What is a new patient in CPT?
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.”. By contrast, an established patient has received professional services from the physician or another physician in ...
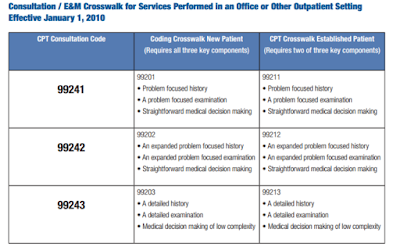
What is a consultation in CPT?
CPT defines a consultation as “a type of service provided by a physician whose opinion or advice regarding evaluation and/or management of a specific problem is requested by another physician or other appropriate source.” For example, if you are asked to see a patient for a pre-operative clearance or for evaluation of a medical problem, the appropriate category might be consultation services. Since the same consultation codes apply to both new and established patients, it is not necessary to apply the new patient definition.
Why is it important to distinguish new patients from established patients?
The reason for learning to distinguish new patients from established patients, apart from following coding guidelines, is that it enables you to be reimbursed for the additional work that new patient visits require (see “Documentation requirements” ).
What is the CPT code for preventive visit?
Preventive visit codes 99381-99397 include “counseling/anticipatory guidance/risk factor reduction interventions,” according to CPT. However, when such counseling is provided as part of a separate problem-oriented encounter, it may be billed using preventive medicine codes 99401-99409.
When is modifier 25 appropriate?
CPT says modifier 25 is appropriate when there is a “significant, separately identifiable evaluation and management service by the same physician on the same day.”. Stated another way, if the second service requires enough additional work that it could stand on its own as an office visit, use modifier 25.
What are preventive visits?
Preventive visits, like many procedural services, are bundled services. Unlike documenting problem-oriented E/M office visits (99201–99215), which involves complicated coding guidelines, documenting preventive visits is more straightforward. The following components are needed: 1 A comprehensive history and physical exam findings; 2 A description of the status of chronic, stable problems that are not “significant enough to require additional work,” according to CPT; 3 Notes concerning the management of minor problems that do not require additional work; 4 Notes concerning age-appropriate counseling, screening labs, and tests; 5 Orders for vaccines appropriate for age and risk factors.
What is the ICd 99381-99397 code?
Preventive visit codes 99381-99397 include “counseling/anticipatory guidance/risk factor reduction interventions,” according to CPT. However, when such counseling is provided as part of a separate problem-oriented encounter, it may be billed using preventive medicine codes 99401-99409. For example, if you provide significant counseling on smoking cessation during a visit for an ankle sprain, you could bill for the counseling in addition to submitting an E/M office visit code for the problem-oriented service. A synopsis of the counseling should be included in your documentation, and ICD-9 codes for preventive counseling should be paired with your CPT codes (see “ Acceptable codes for preventive counseling services ”). Such a visit requires the use of modifier 25.
What is a comprehensive history and physical exam?
A comprehensive history and physical exam findings; A description of the status of chronic, stable problems that are not “significant enough to require additional work,” according to CPT; Notes concerning the management of minor problems that do not require additional work;
What is a new patient?
A new patient is one who has not received any professional services from the physician/qualified health care professional or another physician/qualified health care professional of the exact same specialty and subspecialty who belongs to the same group practice, within the past three years.
How long does it take to determine if a patient is new?
Three-year rule: The general rule to determine if a patient is “new” is that a previous, face-to-face service (if any) must have occurred at least three years from the date of service. Some payers may have different guidelines, such as using the month of their previous visit, instead of the day.
Do all E/M codes fall under the new vs. established categories?
Not all E/M codes fall under the new vs. established categories. For example, in the emergency department (ED), the patient is always new and the provider is always expected to get the patient’s history to diagnose a problem.#N#In the office setting, patients see their provider routinely. The provider knows (or can quickly obtain from the medical record) the patient’s history to manage their chronic conditions, as well as make medical decisions on new problems.#N#A provider seeing a new patient may not have the benefit of knowing the patient’s history. Even if the provider can access the patient’s medical record, they will probably ask more questions.
What is E/M coding?
A persistent concern when reporting evaluation and management (E/M) services is determining whether a patient is new or established to the practice. New patient codes carry higher relative value units (RVUs), and for that reason are consistently under the watchful eye of payers, who are quick to deny unsubstantiated claims. Here are some guidelines that will ensure your E/M coding holds up to claims review.
Popular Posts:
- 1. icd code for osteopenia
- 2. 2016 icd code for groin pain
- 3. icd 10 code for posterior vitreous separation
- 4. icd 10 code for lt shoulder dislocation
- 5. icd 10 code for vaso occlusive crisis
- 6. icd 10 code for right bunion
- 7. icd 10 code for resolved right lower lobe pneumonia
- 8. icd 10 code for mets to bladder
- 9. what is the icd 10 code for aortic root replacement
- 10. icd 10 code for klebsiella pyelonephritis