Procedure and treatment not carried out because of patient's decision for unspecified reasons. Z53. 20 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. The 2022 edition of ICD-10-CM Z53.
What is the code for a primary malignant neoplasm?
What is the Z85 code for a primary malignancy?
What is Chapter 2 of the ICD-10-CM?
What is C80.0 code?
When a pregnant woman has a malignant neoplasm, should a code from subcatego
What is the code for leukemia?
What is C80.1?
See more
About this website
What ICD-10 code to use for no diagnosis?
2. ICD-10 Code Z03. 89: No Diagnosis. The description is changed from “No Diagnosis” to “Encounter for observation for other suspected diseases and conditions ruled out.” Examples for use of Z03.
What is the ICD-10 code for cancer unspecified?
ICD-10-CM Code for Malignant (primary) neoplasm, unspecified C80. 1.
What is diagnosis code Z51 11?
ICD-10 code Z51. 11 for Encounter for antineoplastic chemotherapy is a medical classification as listed by WHO under the range - Factors influencing health status and contact with health services .
What is diagnosis code Z08?
ICD-10 code: Z08 Follow-up examination after treatment for malignant neoplasm.
What does unspecified cancer mean?
Cancer of unknown primary (CUP) means that cancer spread has been found in your body (secondary cancer), but your doctors can't find where the cancer started (the primary cancer). It is sometimes called unknown primary cancer or unknown primary tumour.
What is considered active cancer treatment?
Treatment given to cure the cancer, such as chemotherapy or radiation therapy. This does not include long-term treatment such as hormone medication, which may be taken for several years to maintain remission.
What is admin code 96413?
96413. Chemotherapy administration, intravenous infusion technique, up to 1 hour, single or initial substance drug.
What is the ICD-10 PCS code for chemotherapy?
2022 ICD-10-PCS Procedure Code 3E03305: Introduction of Other Antineoplastic into Peripheral Vein, Percutaneous Approach.
What is the ICD-10 code for History of radiation therapy?
ICD-10 Code for Personal history of irradiation- Z92. 3- Codify by AAPC.
What is the ICD-10 code for adverse effect of chemotherapy?
ICD-10-CM Code for Adverse effect of antineoplastic and immunosuppressive drugs, initial encounter T45. 1X5A.
What is the ICD-10 for CAD?
Code I25* is the diagnosis code used for Chronic Ischemic Heart Disease, also known as Coronary artery disease (CAD). It is a is a group of diseases that includes: stable angina, unstable angina, myocardial infarction, and sudden coronary death.
What is primary malignant neoplasm?
A malignant tumor at the original site of growth. [ from NCI]
2021 ICD-10-CM Guidelines
ICD-10-CM Official Guidelines for Coding and Reporting FY 2021 (October 1, 2020 - September 30, 2021) Narrative changes appear in bold text . Items underlined have been moved within the guidelines since the FY 2020 version
2022 ICD-10-PCS Official Guidelines for Coding and Reporting
Amputation of the foot is coded to the root operation Detachment in the body system Anatomical Regions, Lower Extremities. B2.1b . Where the general body part values “upper” and “lower” are provided as an option in the
ICD-10-CM Official Guidelines for Coding and Reporting
ICD-10-CM Official Guidelines for Coding and Reporting FY 2019 (October 1, 2018 - September 30, 2019) Narrative changes appear in bold text . Items underlined have been moved within the guidelines since the FY 2018 version
ICD-10 coding for suspected cancer
If a neoplasm is unconfirmed, code the sign or symptom. (See below under uncertain diagnosis). And, keep in mind the ICD-10 coding rules for reporting confirmed neoplasms.
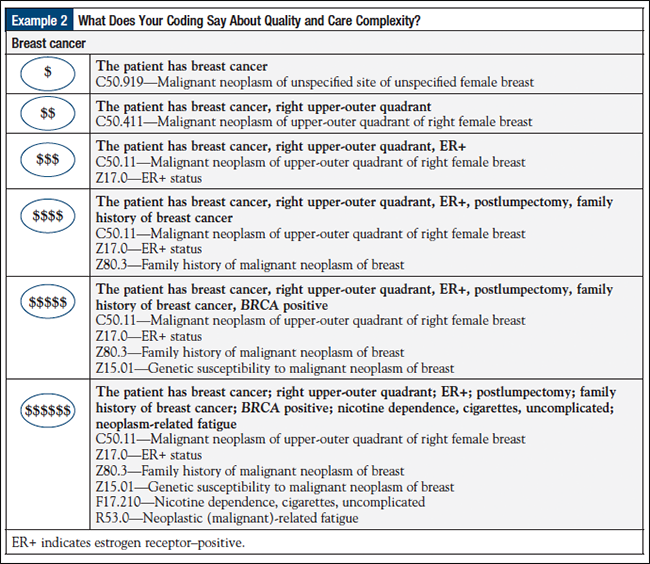
CORRECTLY CODING: BREAST, PROSTATE, AND OTHER CANCERS AND TUMORS
CORRECTLY CODING: BREAST, PROSTATE, AND OTHER CANCERS AND TUMORS When selecting International Classification of Diseases, Tenth Revision (ICD-10) diagnostic codes, accuracy is important when
Clear Up Confusion as to When Cancer Becomes “History Of”
I’d like to thank Emily for such a clear, concise reckoning on when to code ‘history of’ cancer. As a Clinical Documentation Improvement specialist in the Oncology setting, I come across this topic quite often.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
What is the table of neoplasms used for?
The Table of Neoplasms should be used to identify the correct topography code. In a few cases, such as for malignant melanoma and certain neuroendocrine tumors, the morphology (histologic type) is included in the category and codes. Primary malignant neoplasms overlapping site boundaries.
What does "type 1 excludes" mean?
A type 1 excludes note is for used for when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
What is the difference between leukemia and sarcoma?
Sarcoma is a malignancy that begins in bone, cartilage, fat, muscle, blood vessels, or other connective or supportive tissue. Leukemia is a malignancy that starts in blood-forming tissue such as the bone marrow, and causes large numbers of abnormal blood cells to be produced and enter the blood.
When to use a malignant neoplasm code?
Use a malignant neoplasm code if the patient has evidence of the disease, primary or secondary, or if the patient is still receiving treatment for the disease. If neither of those is true, then report personal history of malignant neoplasm.
What is the code for primary malignancy?
When a primary malignancy has been previously excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy .
What is an uncertain diagnosis?
Uncertain diagnosis. Do not code diagnoses documented as “probable”, “suspected,” “questionable,” “rule out,” or “working diagnosis” or other similar terms indicating uncertainty. Rather, code the condition (s) to the highest degree of certainty for that encounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit. ...
Why is Z53.09 not carried out?
Z53.09 Procedure and treatment not carried out because of other contraindication. Z53.1 Procedure and treatment not carried out because of patient's decision for reasons of belief and group pressure. Z53.2 Procedure and treatment not carried out because of patient's decision for other and unspecified reasons.
What is a Z00-Z99?
Categories Z00-Z99 are provided for occasions when circumstances other than a disease, injury or external cause classifiable to categories A00 -Y89 are recorded as 'diagnoses' or 'problems'. This can arise in two main ways:
What is the ICd 10 code for cancer?
For more context, consider the meanings of “current” and “history of” (ICD-10-CM Official Guidelines for Coding and Reporting; Mayo Clinic; Medline Plus, National Cancer Institute):#N#Current: Cancer is coded as current if the record clearly states active treatment is for the purpose of curing or palliating cancer, or states cancer is present but unresponsive to treatment; the current treatment plan is observation or watchful waiting; or the patient refused treatment.#N#In Remission: The National Cancer Institute defines in remission as: “A decrease in or disappearance of signs or symptoms of cancer. Partial remission, some but not all signs and symptoms of cancer have disappeared. Complete remission, all signs and symptoms of cancer have disappeared, although cancer still may be in the body.”#N#Some providers say that aromatase inhibitors and tamoxifen therapy are applied during complete remission of invasive breast cancer to prevent the invasive cancer from recurring or distant metastasis. The cancer still may be in the body.#N#In remission generally is coded as current, as long as there is no contradictory information elsewhere in the record.#N#History of Cancer: The record describes cancer as historical or “history of” and/or the record states the current status of cancer is “cancer free,” “no evidence of disease,” “NED,” or any other language that indicates cancer is not current.#N#According to the National Cancer Institute, for breast cancer, the five-year survival rate for non-metastatic cancer is 80 percent. The thought is, if after five years the cancer isn’t back, the patient is “cancer free” (although cancer can reoccur after five years, it’s less likely). As coders, it’s important to follow the documentation as stated in the record. Don’t go by assumptions or averages.
What is the ICd 10 code for primary malignancy?
According to the ICD-10 guidelines, (Section I.C.2.m):#N#When a primary malignancy has been excised but further treatment, such as additional surgery for the malignancy, radiation therapy, or chemotherapy is directed to that site, the primary malignancy code should be used until treatment is complete.#N#When a primary malignancy has been excised or eradicated from its site, there is no further treatment (of the malignancy) directed to that site, and there is no evidence of any existing primary malignancy, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy.#N#Section I.C.21.8 explains that when using a history code, such as Z85, we also must use Z08 Encounter for follow-up examination after completed treatment for a malignant neoplasm. This follow-up code implies the condition is no longer being actively treated and no longer exists. The guidelines state:#N#Follow-up codes may be used in conjunction with history codes to provide the full picture of the healed condition and its treatment.#N#A follow-up code may be used to explain multiple visits. Should a condition be found to have recurred on the follow-up visit, then the diagnosis code for the condition should be assigned in place of the follow-up code.#N#For example, a patient had colon cancer and is status post-surgery/chemo/radiation. The patient chart notes, “no evidence of disease” (NED). This is reported with follow-up code Z08, first, and history code Z85.038 Personal history of other malignant neoplasm of large intestine, second. The cancer has been removed and the patient’s treatment is finished.
What is preventative cancer?
Preventative or Prophylactic – to keep cancer from reoccurring in a person who has already been treated for cancer or to keep cancer from occurring in a person who has never had cancer but is at increased risk for developing it due to family history or other factors.
Does history of cancer affect relative value units?
The fear is, history of will be seen as a less important diagnosis, which may affect relative value units . Providers argue that history of cancer follow-up visits require meaningful review, examinations, and discussions with the patients, plus significant screening and watching to see if the cancer returns.
Is cancer history?
History of Cancer: The record describes cancer as historical or “history of” and/or the record states the current status of cancer is “cancer free,” “no evidence of disease,” “NED,” or any other language that indicates cancer is not current. According to the National Cancer Institute, for breast cancer, the five-year survival rate ...
Do providers look at cancer at the cellular level?
According to a presentation by James M. Taylor, MD, CPC, providers look at cancer at a cellular level; whereas, coding guidelines look more at the organ level. In his opinion, common concerns among providers are: Some neoplasms may not be active but remain at a cellular level, and can become active.
What is the code for a primary malignant neoplasm?
A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion '), unless the combination is specifically indexed elsewhere. For multiple neoplasms of the same site that are not contiguous such as tumors in different quadrants of the same breast, codes for each site should be assigned.
What is the Z85 code for a primary malignancy?
When a primary malignancy has been previously excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy at that site, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy. Any mention of extension, invasion, or metastasis to another site is coded as a secondary malignant neoplasm to that site. The secondary site may be the principal or first-listed with the Z85 code used as a secondary code.
What is Chapter 2 of the ICD-10-CM?
Chapter 2 of the ICD-10-CM contains the codes for most benign and all malignant neoplasms. Certain benign neoplasms , such as prostatic adenomas, may be found in the specific body system chapters. To properly code a neoplasm, it is necessary to determine from the record if the neoplasm is benign, in-situ, malignant, or of uncertain histologic behavior. If malignant, any secondary ( metastatic) sites should also be determined.
What is C80.0 code?
Code C80.0, Disseminated malignant neoplasm, unspecified, is for use only in those cases where the patient has advanced metastatic disease and no known primary or secondary sites are specified. It should not be used in place of assigning codes for the primary site and all known secondary sites.
When a pregnant woman has a malignant neoplasm, should a code from subcatego
When a pregnant woman has a malignant neoplasm, a code from subcategory O9A.1 -, malignant neoplasm complicating pregnancy, childbirth, and the puerperium, should be sequenced first, followed by the appropriate code from Chapter 2 to indicate the type of neoplasm. Encounter for complication associated with a neoplasm.
What is the code for leukemia?
There are also codes Z85.6, Personal history of leukemia, and Z85.79, Personal history of other malignant neoplasms of lymphoid, hematopoietic and related tissues. If the documentation is unclear as to whether the leukemia has achieved remission, the provider should be queried.
What is C80.1?
Code C80.1, Malignant ( primary) neoplasm, unspecified, equates to Cancer, unspecified. This code should only be used when no determination can be made as to the primary site of a malignancy. This code should rarely be used in the inpatient setting.

Popular Posts:
- 1. what would be the appropriate icd-10-cm code for lumbar stenosis?
- 2. what is the icd 10 code for history of tia
- 3. icd 10 cm code for active labor frank breech
- 4. icd 10 code for cervical dysplasia
- 5. icd code 10 for wound check
- 6. icd 10 code for pushed down by another person
- 7. icd-10 code for q93.5
- 8. icd-10-pcs code for acute nephritis syndrome with diffuse crescentic glomerulonephrtitis
- 9. icd code for hx spinal stenosis
- 10. icd 10 code for encounter for nasogastric (ng) tube placement