If a patient has not previously been diagnosed with diabetes and is being seen for a screening, it is not appropriate to assign a diabetic diagnosis. You would assign ICD-10 code Z13. 1, Encounter for screening for diabetes mellitus.
Full
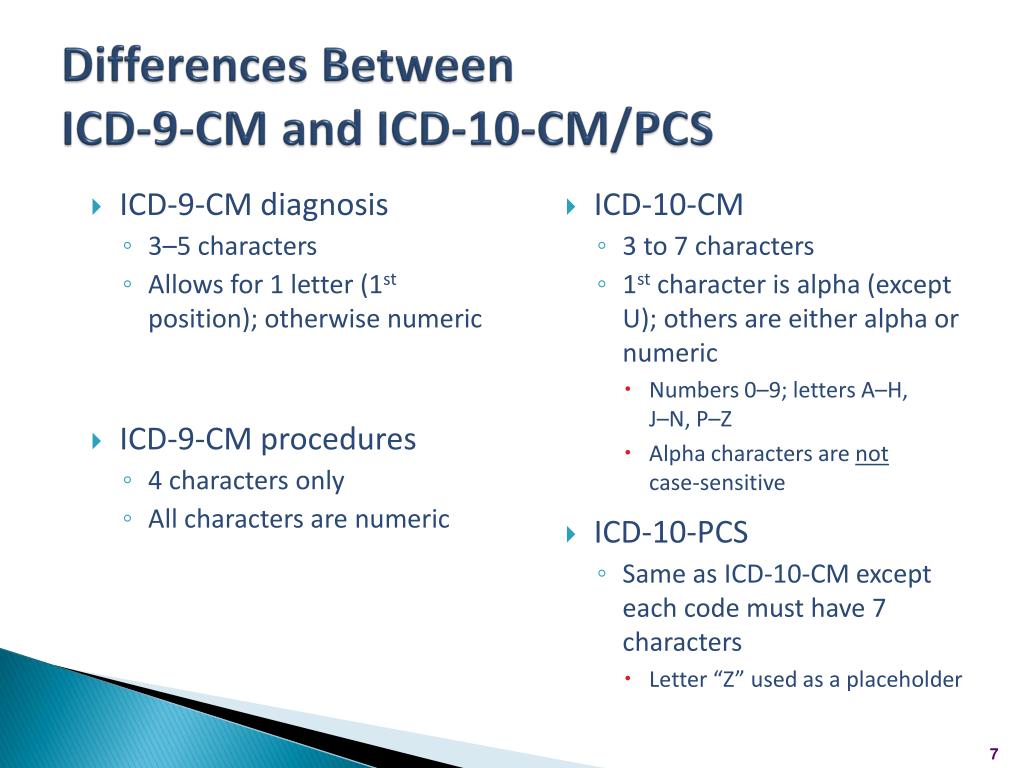
AnswerWhat is the ICD 9 code for diabetes mellitus DM?
DM is assigned to ICD-9-CM category 250. Secondary diabetes is classified to category 249. When the physician documents DM, additional documentation is necessary to completely classify the condition: type 1 vs. type 2, uncontrolled vs. controlled, and manifestations associated with the condition, if any.
What is the ICD 10 code for screening for diabetes mellitus?
You would assign ICD-10 code Z13.1, Encounter for screening for diabetes mellitus. This code can be found under “Screening” in the Alphabetical Index of the ICD-10 book. If a member has been diagnosed with prediabetes, or has had a previous diagnosis of diabetes and the disease is now considered
What are the ICD-10-CM coding guidelines?
The ICD-10-CM coding guidelines established by the National Center for Health Care (NCHC) and the Centers for Medicare & Medicaid Services (CMS) for ICD-10-CM assist healthcare professionals and medical coders in selecting the appropriate diagnosis codes to report for a specific patient encounter.
What is the ICD 10 code for dormant diabetes?
latent or dormant (per the provider’s documentation) the ICD-10 code R73.09, Other abnormal glucose, should be assigned. This code can be found under “Diabetes” and then “latent,” or under “Abnormal” and then “glucose” in the Alphabetical Index of the. ICD-10 book.
What's the default if the physician does not document the type of diabetes?
The guidelines state that if the type of diabetes is not documented, the default is type 2. The guidelines also instruct to use additional codes to identify long-term control with insulin (Z79. 4) or oral hypoglycemic drugs (Z79.
What is the ICD-10 code for pre DM?
The ICD-10 code for prediabetes is R73. 09.
What codes are used when the documentation provided by the provider is insufficient?
Codes titled "unspecified" are for use when the information in the medical record is insufficient to assign a more specific code.
What is the ICD code for DM?
Diabetes mellitus (E10-E14)CodeTitle.0With coma Incl.: Diabetic: coma with or without ketoacidosis hyperosmolar coma hypoglycaemic coma Hyperglycaemic coma NOS.1With ketoacidosis Incl.: Diabetic: acidosis ketoacidosis without mention of coma8 more rows
What is the ICD-10 code for type 2 diabetes?
ICD-Code E11* is a non-billable ICD-10 code used for healthcare diagnosis reimbursement of Type 2 Diabetes Mellitus. Its corresponding ICD-9 code is 250. Code I10 is the diagnosis code used for Type 2 Diabetes Mellitus.
What is DX code e785?
Hyperlipidemia, UnspecifiedCode E78. 5 is the diagnosis code used for Hyperlipidemia, Unspecified, a disorder of lipoprotein metabolism other lipidemias. It is a condition with excess lipids in the blood.
How should you respond to inadequate documentation while coding?
How Should You Respond To Inadequate Documentation While Coding. Make your workflow more efficient. It is imperative you establish two-way communication with the coders… Communicate using the standard method.
What does insufficient documentation mean?
No documentation of intent to order services and procedures (for example, incomplete or missing signed order or progress note describing intent for services to be provided).
What diagnosis codes Cannot be primary?
Diagnosis Codes Never to be Used as Primary Diagnosis With the adoption of ICD-10, CMS designated that certain Supplementary Classification of External Causes of Injury, Poisoning, Morbidity (E000-E999 in the ICD-9 code set) and Manifestation ICD-10 Diagnosis codes cannot be used as the primary diagnosis on claims.
What is Type 2 diabetes mellitus without complications ICD-10?
ICD-10 code: E11. 9 Type 2 diabetes mellitus Without complications.
What is the proper ICD-10 code for Type 2 diabetes mellitus with multiple complications?
E11. 69 - Type 2 diabetes mellitus with other specified complication. ICD-10-CM.
What is the ICD-10 code for type 2 diabetes on insulin?
Certain conditions have both an underlying etiology and multiple body system manifestations due to the underlying etiology. For such conditions the ICD-10-CM has a coding convention that requires the underlying condition be sequenced first followed by the manifestation.
What does CPT code 99241 mean?
CPT® Code 99241 - New or Established Patient Office or Other Outpatient Consultation Services - Codify by AAPC. CPT. Evaluation and Management Services. Consultation Services. Office or Other Outpatient Consultation Services.
What does CPT code 99244 mean?
CPT Code Description 99244 Office consultation for a new or established patient, which requires these 3 key components: A comprehensive history; A comprehensive examination; and Medical decision making of moderate complexity.
What does CPT code 99251 mean?
99251: Inpatient consultation, which requires these three key components: A problem-focused history; A problem-focused examination; and. Straightforward medical decision-making.
When do you use modifier 32?
When to use Modifier 32. Modifier -32 indicates a service that is required by a third-party entity, Worker's Compensation, or some other official body. Modifier 32 is no used to report a second opinion request by a patient, a family member or another physician. This modifier is used only when a service is mandated.
Why is diagnosis coding important?
Diagnosis coding is very important for any specialty, and coding should be performed at the highest level of specificity. Coding and documentation should tell the payor what us going on, and why. Evidence in the documentation should identify clearly what services were performed and the reasons.
What is EHR in healthcare?
The electronic health record (EHR) can be help or a hindrance when selecting a diagnosis code. For one practice I visited, when they typed in the diagnosis of “thrombosis,” all the available diagnoses were presented as a pick list, with the unspecified code listed first.
When should specific diagnosis codes be reported?
While specific diagnosis codes should be reported when they are supported by the available medical record documentation and clinical knowledge of the patient’s health condition , there are instances when signs/symptoms or unspecified codes are the best choices for accurately reflecting the healthcare encounter.
Why is it important to report co-morbid conditions?
By reporting the co-morbid conditions that affect patient management, it helps to ensure that the services provided are supported by medical necessity. However, the conditions must be documented in the medical record. If not documented, then the conditions cannot be reported.
When sufficient clinical information isn’t known or available about a particular health condition to assign a more specific answer
When sufficient clinical information isn’t known or available about a particular health condition to assign a more specific code, it is acceptable to report the appropriate unspecified code (e.g., a diagnosis of pneumonia has been determined, but not the specific type).
When should unspecified codes be reported?
Unspecified codes should be reported when they are the codes that most accurately reflect what is known about the patient’s condition at the time of that particular encounter. Another issue that comes up frequently is that if the physician is not managing a co-morbid condition, they do not report a comorbid diagnosis.
Can you use keywords in an EHR?
Of course, it’s the unspecified diagnosis. If you are using your EHR to select your diagnosis, make sure you build smart phrases or keywords to help narrow down the selection to a more specific diagnosis. If you have not built keywords or phrases, now is the time to start.
Type 2 Diabetes Mellitus With Other Specified Complication
Diabetes mellitus, type 2 with ketoacidotic coma Diabetes type 2 low hdl and high triglyceride Diabetes type 2 with erectile dysfunction Diabetes type 2 with hyperlipidemia Diabetes type 2 with severe malnutrition Diabetes, type 2 with ketoacidosis Diabetes, type 2 with osteomyelitis Dyslipidemia with high density lipoprotein below reference range and triglyceride above reference range due to type 2 diabetes mellitus Erectile dysfunction associated with type 2 diabetes mellitus Hyperlipidemia due to type 2 diabetes mellitus Ketoacidosis in type 2 diabetes mellitus Ketoacidosis in type ii diabetes mellitus Ketoacidotic coma in type 2 diabetes mellitus Ketoacidotic coma in type ii diabetes mellitus Mixed hyperlipidemia associated with type 2 diabetes mellitus Mixed hyperlipidemia due to type 2 diabetes mellitus Osteomyelitis due to type 2 diabetes mellitus Severe malnutrition due to type 2 diabetes mellitus Continue reading >>.
Linking.... Acdis Forums
We recently had a recent topic come up with our CDI's and physician advisor and I am hoping to get some guidance on the issue. The question came up when we were doing a group chart review on a record where the coder had asked for multiple retro queries. The patient was admitted with PAD with limb ischemia with dry gangrene.
Coding Diabetes Mellitus With Associated Conditions
Overseen by AHIMA’s coding experts for the Journal of AHIMA website, the Code Cracker blog takes a look at challenging areas and documentation opportunities for coding and reimbursement. Check in each month for a new discussion.
Diabetes And Osteomyelitis In Icd 10
If this is your first visit, be sure to check out the FAQ & read the forum rules . To view all forums, post or create a new thread, you must be an AAPC Member . If you are a member and have already registered for member area and forum access , you can log in by clicking here .
Coding For Diabetes Mellitus
For The Record Vol. 23 No. 19 P. 27 In type 1 diabetes mellitus (DM), beta cells are destroyed by an autoimmune process that usually leads to a complete loss of insulin production. The majority of patients who develop type 1 DM will do so prior to age 25, with an increased prevalence due to heredity or in patients with other autoimmune diseases.
Coding Clinic Solves Documentation Issues, Changes Paradigm For Diabetes And Heart Failure Coding
Coding Clinic Solves Documentation Issues, Changes Paradigm for Diabetes and Heart Failure Coding By Allen R.
Coding Tip: Dm With Assumed Conditions
Diabetes continues to be a challenge for coders since the new instruction/guideline was released in AHA Coding Clinic for ICD-10-CM and ICD-10-PCS, First Quarter 2016. This is effective with March 18, 2016 discharges. ICD-10-CM does assume the link between diabetes and multiple common conditions.
What is the code for charcots arthropathy?
Here is one for you.. Provider chose code A52.16 for Charcots arthropathy., in the assessment and plan portion of the note. The problem is since that is the code and description inserted into the assessment, that is the code the coder put on the claim. when it was then disputed (with my help) the coder adamantly stated this was the diagnosis assigned by the provider. The only problem is , it was not. The provider in the exam and discussion clearly intended this to be charcots arthropathy of the ankle due to diabetes which is an entirely different code. this patient has never had syphllis which is the basis for A52.16. The provider had no idea because he only saw the number and the standardized description and did not know. this is the problem with using the standard code number with description from the book,. The providers narrative must be the diagnosis
Can ICD-10 be used in acute care?
If a doctor documents a critical care code only to be used in an acute care setting, and he doesn't document the patient going right to the hospital, then, no, don't capture that, even if it is the A/P.
Who can correct a medical record?
Only the attending physician can correct the medical record. The amendment should be based on an observation of the patient on the date of service and be signed by the observing physician (e.g., a follow-up note based on a diagnostic test ordered and test results received subsequent to the patient visit).
What is a late entry in medical records?
A late entry, an addendum or a correction to the medical record, bears the current date of that entry and is signed by the person making the addition or change. Late Entry: A late entry supplies additional information that was omitted from the original entry.
What is correction in electronic records?
When a hard copy is generated from an electronic record, both records must show the correction.
Why do hospitals use physician queries?
Physician Queries – Queries are often used in hospitals to achieve compliant documentation and appropriate diagnostic related groups (DRGs). The Center for Medicare & Medicaid Services (CMS) has adopted query guidance for hospital needs, but there is nothing in the guidance to indicate queries are only for hospitals.
Who must document HPI?
According to CMS, the history of present illness (HPI) must be documented by the physician, and cannot be documented by the ancillary staff. As an auditor, I see this being documented by the medical assistant often, and that is not appropriate.
Do auditors have to be aware of the documentation rules?
Auditors are bound by the documentation rules, and physicians need to be aware that those rules are for the protection of the patient in the completeness of the record – but also to assist the physician as a prompt during the encounter with the patient.
Popular Posts:
- 1. icd 10 code for fracture of sacrum
- 2. icd 9 code for left trapisus strain
- 3. icd 10 code for metastatic carcinoma of the left breast to bone
- 4. icd 10 code for bmi 45.3
- 5. icd 10 cm code for hot coal
- 6. icd 10 code for aftercare left hip hemiarthroplasty
- 7. icd 10 code for high level of care
- 8. icd 10 code for calculus of gallbladder
- 9. what is the icd 10 code for spinal fusion
- 10. icd 10 code for renaldisease