It is appropriate to list as a secondary diagnosis the specific infection, if documented, such as sepsis. Therefore, sepsis due to a peripherally inserted central catheter (PICC) line is assigned to codes 999.32, 038.9, and 995.91.Oct 22, 2012
Full
AnswerWhat is the CPT code for sepsis with a PICC line?
It is appropriate to list as a secondary diagnosis the specific infection, if documented, such as sepsis. Therefore, sepsis due to a peripherally inserted central catheter (PICC) line is assigned to codes 999.32, 038.9, and 995.91.
What is the ICD 10 code for PICC line?
Z45. 2 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. Is a PICC line an infusion device? This is one of the most common questions that patients have when they are told that they need home infusions.
What is the ICD 10 code for sepsis?
Coding tips: In ICD-10-CM, only one code is needed to report sepsis without organ dysfunction. Most sepsis codes can be found in A40.- through A41.9.
What is the CPT code for sepsis with E coli?
If the physician specifies a causal organism, such as “sepsis due to E. Coli,” “sepsis with blood cultures positive for E. Coli,” or “E. Coli sepsis,” use the code for sepsis naming the specific organism. The category A40.- through A41.9 is for sepsis due to bacteria or unspecified bacteria.
What is the ICD-10 PCS code for PICC?
Insertion of Infusion Device into Left Internal Jugular Vein, Percutaneous Approach. ICD-10-PCS 05HN33Z is a specific/billable code that can be used to indicate a procedure.
What is the ICD-10 code for PICC line complication?
T82.594Other mechanical complication of infusion catheter The 2022 edition of ICD-10-CM T82. 594 became effective on October 1, 2021.
What is the 2021 ICD-10 code for sepsis?
ICD-10 code A41. 9 for Sepsis, unspecified organism is a medical classification as listed by WHO under the range - Certain infectious and parasitic diseases .
What is the ICD-10 code for sepsis?
Septicemia – There is NO code for septicemia in ICD-10. Instead, you're directed to a combination 'A' code for sepsis to indicate the underlying infection, such A41. 9 (Sepsis, unspecified organism) for septicemia with no further detail.
What is the ICD 10 code for PICC line insertion?
Encounter for adjustment and management of implanted device ICD-10-CM Z45.
What is the ICD 10 code for attention to PICC line?
Z45.2Z45. 2 - Encounter for adjustment and management of vascular access device | ICD-10-CM.
What is urosepsis ICD-10 code?
Urosepsis Is No Longer Coded Considered in ICD-10-CM as a nonspecific term and not associated with sepsis, the default code for this condition in ICD-9-CM (599.0 Urinary tract infection, site not specified) is not carried forward in ICD-10-CM.
When do you code sepsis as a principal diagnosis?
Coding sepsis requires a minimum of two codes: a code for the systemic infection (e.g., 038. xx) and the code 995.91, SIRS due to infectious process without organ dysfunction. If no causal organism is documented within the medical record, query the physician or assign code 038.9, Unspecified septicemia.
What is the ICD-10 code for severe sepsis with septic shock?
ICD-10 code R65. 21 for Severe sepsis with septic shock is a medical classification as listed by WHO under the range - Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified .
Is sepsis coded first?
When sepsis is present on admission and due to a localized infection (not a device or post procedural), the sepsis code is sequenced first followed by the code for the localized infection.
What is other specified sepsis?
89 for Other specified sepsis is a medical classification as listed by WHO under the range - Certain infectious and parasitic diseases .
What is the diagnosis for ICD-10 code R50 9?
ICD-10 | Fever, unspecified (R50. 9)
What is the ICd 10 code for a catheter?
Local infection due to central venous catheter 1 T80.212 should not be used for reimbursement purposes as there are multiple codes below it that contain a greater level of detail. 2 The 2021 edition of ICD-10-CM T80.212 became effective on October 1, 2020. 3 This is the American ICD-10-CM version of T80.212 - other international versions of ICD-10 T80.212 may differ.
What is the secondary code for Chapter 20?
Use secondary code (s) from Chapter 20, External causes of morbidity, to indicate cause of injury. Codes within the T section that include the external cause do not require an additional external cause code. Type 1 Excludes.
What is post-procedural sepsis?
Post-procedural Sepsis and Sepsis Due to a Device, Implant, or Graft. A systemic infection can occur as a complication of a procedure or due to a device, implant, or graft. This includes systemic infections due to wound infection, infusions, transfusions, therapeutic injections, implanted devices, and transplants.
Why is severe sepsis not assigned?
For instance, if severe sepsis, pneumonia, and acute renal failure due to dehydration are documented, the code for severe sepsis may not be assigned because the acute renal failure is not stated as due to or associated with sepsis. If the documentation is unclear, query the physician.
What is the A41.51?
A41.51 Sepsis due to Escherichia coli [E. coli] N39.0. SIR S. SIRS is the body’s clinical cascading response to infection or trauma that triggers an acute inflammatory reaction and progresses to coagulation of the blood, impaired fibrinolysis, and organ failure.
What is the P36 code?
Codes from category P36 include the organism; an additional code for the infectious organism is not assigned. If the P36 code does not describe the specific organism, an additional code for the organism can be assigned. Urosepsis. The term “urosepsis” is not coded in ICD-10-CM.
When to add R65.2-?
If the patient has severe sepsis, add R65.2- with the codes for specific organ dysfunctions.
When to query a physician for sepsis?
You must query the physician when the term “sepsis syndrome” is documented as a final diagnosis. Know when to Query. Sepsis is a complicated condition to code, and it is often necessary to query the physician to code the case correctly.
Can a localized infection cause tachycardia?
Documentation issues: Often, a patient with a localized infection may exhibi t tachycardia, leukocytosis, tachypnea, and fever, but not truly have SIRS or sepsis. These are typical symptoms of any infection. It’s up to the physician’s clinical judgment to decide whether the patient has sepsis or SIRS.
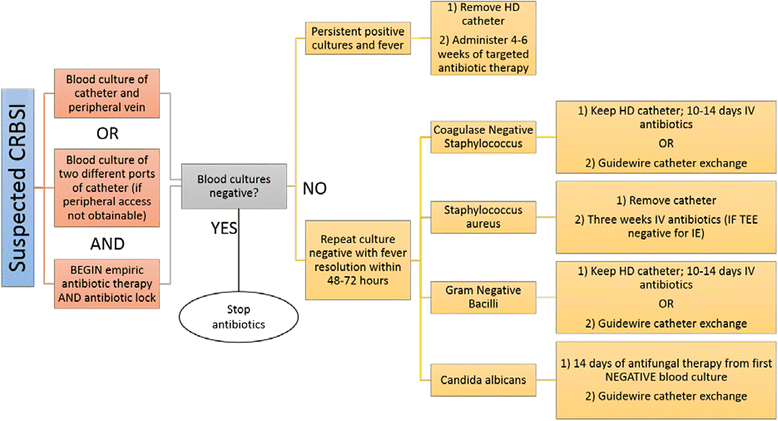
What are the two major categories of infections due to central venous catheters?
There are two major categories of infections due to central venous catheters: local and systemic . Local infections include exit or insertion site, port or reservoir, and tunnel infections. Systemic infections may be documented as central line-associated bloodstream infections (CLABSIs).
Why is it important to assign codes to physicians?
Because of the implications the presence of these codes may cause , it is vitally important that coders assign them accurately and consistently based on physician documentation and supportive clinical evidence in the medical record. It may be necessary to query the physician for clarification.
Can a coder assume a link between a catheter and a UTI?
If a patient is admitted with an indwelling catheter and is noted to have a urinary tract infection (UTI), the coder should not assume a link between the catheter and the UTI. The physician must clearly document the causal relationship before code 996.64 can be assigned.
Is coding and sequencing for catheter infections dependent on the physician documentation in the medical record?
It may be necessary to query the physician for clarification. Coding and sequencing for catheter infections are dependent on the physician documentation in the medical record and application of the Official Coding Guidelines for inpatient care.
Popular Posts:
- 1. icd 10 code for 24 hour urine collection
- 2. icd 10 code for procedure inserts an anterior nasal packing into left nostril
- 3. icd 10 code for toothl abscess
- 4. icd 10 code for chronic bph
- 5. icd-10 code for stomatitis
- 6. icd 10 code for ovarian masses teratoma
- 7. icd 10 code for altered mental status due to overdose
- 8. icd 10 code for l otitis externa
- 9. icd 9 code for cervical kyphosis
- 10. icd 10 code for scratches on skin